Pelvic organ prolapse (POP) is a condition where one or more organs in the pelvis, such as the bladder, uterus (or vaginal vault, in women with previous hysterectomy), or rectum, descend into the vaginal space due to weakened pelvic floor muscles and connective tissues. While POP cannot be fully reversed [1], various treatment options are available to improve POP/prevent it from worsening, manage symptoms and improve overall quality of life.
Pelvic organ prolapse occurs when one or more pelvic organs descend into the vaginal space due to weakened pelvic floor muscles and connective tissues.
What causes pelvic organ prolapse?
Pelvic organ prolapse (POP) occurs when the pelvic floor muscles and connective tissues weaken or become damaged [2]. Some of the following risk factors can contribute to the development of pelvic organ prolapse:
Pregnancy and childbirth: pregnancy with a growing foetus in one’s uterus increases the intra-abdominal pressure, which is in turn transmitted to the pelvic floor. Women with multiple pregnancies and big babies are at even higher risk [3,4]. Raised intra-abdominal pressures throughout pregnancy stretch the pelvic floor muscles and lead to weakening. The process of childbirth, particularly vaginal delivery and instrumental (assisted vaginal delivery, where a vacuum/forceps is used to assist in the delivery of the baby), involves significant strain on the pelvic floor muscles and supporting structures, which can stretch, tear, and get damaged during the process. Lack of proper rehabilitation/pelvic floor exercises in antenatal and postpartum may also weaken the pelvic floor muscles [5].
Ageing: as women age and reach menopause, the pelvic floor muscles and supportive tissues naturally weaken and lose elasticity. Menopause also sees a significant decline in oestrogen levels in women. These age-related changes reduce the ability of these tissues to provide adequate support for the pelvic organs, increasing the risk of having a pelvic organ prolapse. Older women are also more prone to chronic health conditions, some of which may predispose one to pelvic organ prolapse; these include obesity, chronic cough, and constipation, all of which can exert additional strain on the pelvic floor muscles and tissues. However, not all individuals will experience pelvic organ prolapse as they age, and preventive measures such as pelvic floor exercises and healthy lifestyle habits can help reduce the risk [6].
Lifestyle factors: activities that involve chronic straining or increased intra-abdominal pressure, such as heavy lifting, chronic constipation, or repetitive high-impact activities, can stress the pelvic floor and increase the risk of prolapse [7].
Connective tissue disorders: in some individuals, certain connective tissue disorders, such as Ehlers-Danlos syndrome or Marfan syndrome, can weaken the supportive structures of the pelvis as these conditions typically affect connective tissue strength and pelvic floor support and, in turn, increase the susceptibility to pelvic organ prolapse, which may present/manifest at a relatively younger age.
Obesity: excess weight (particularly truncal obesity) also leads to increased intra-abdominal pressures pressure, which chronically/continuously places additional stress/strain on the pelvic floor muscles and supporting structures, leading to gradual weakening/damage over time and increasing one’s risk factor for pelvic organ prolapse [8].
Previous pelvic surgery: prior pelvic surgery, e.g. surgeries involving the removal of the uterus (hysterectomy), can disrupt the normal pelvic anatomy and weaken the supportive structures, resulting in a slightly increased risk of subsequent pelvic organ prolapse [9]; it is hence important to discuss with your surgeon regarding prophylactic measures that can reduce this risk in the future.
Childbirth, particularly vaginal delivery, can contribute to pelvic organ prolapse by stretching and weakening the pelvic floor muscles and connective tissues.
What are the different types of pelvic organ prolapse and its symptoms?
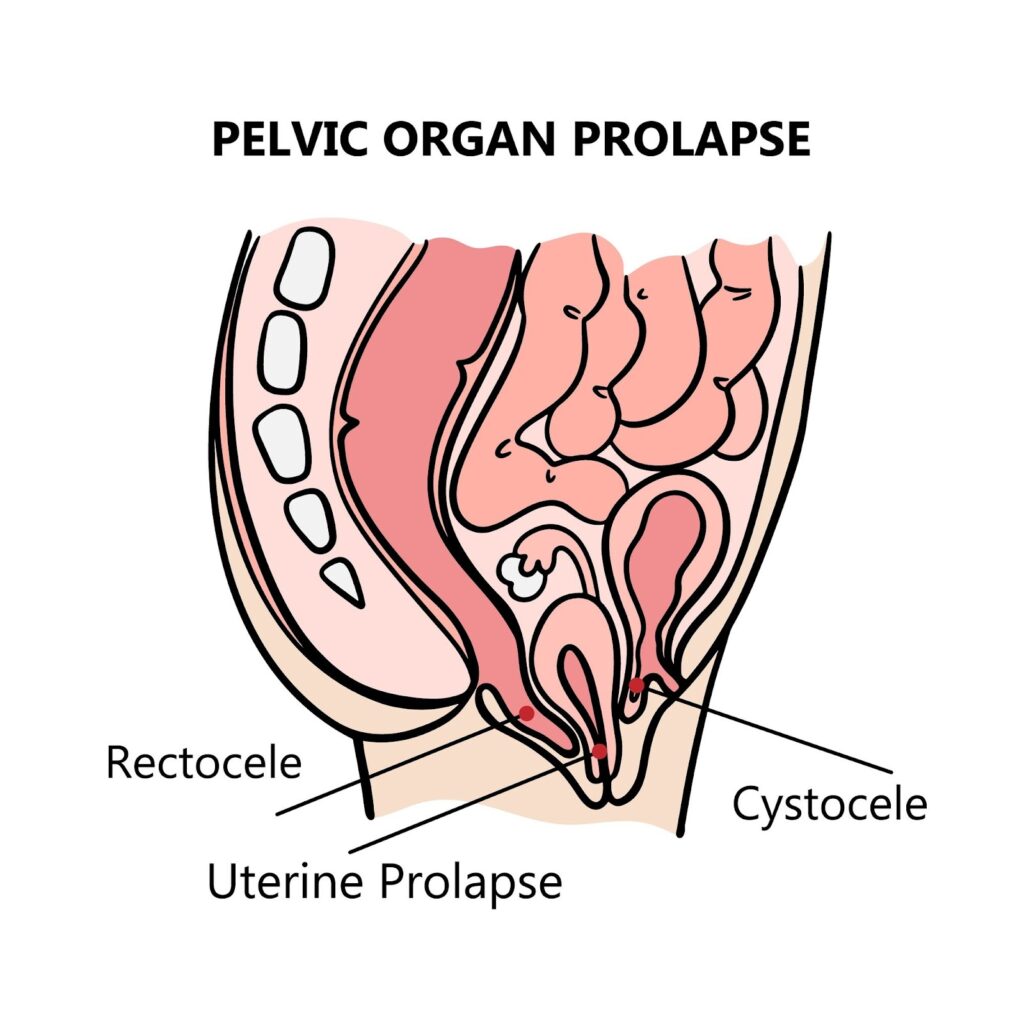
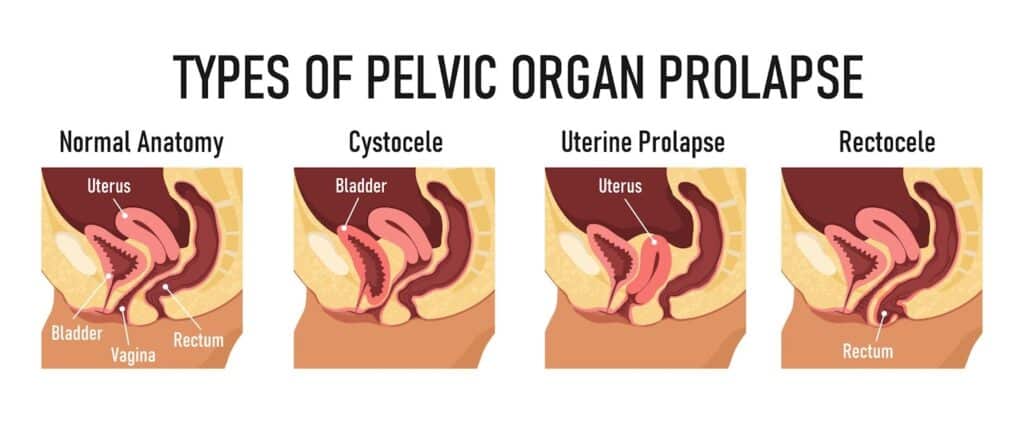
Pelvic organ prolapse (POP) can involve various pelvic organs descending into the vaginal space due to weakened or damaged pelvic floor muscles and connective tissues. The specific type of prolapse depends on which organ or organs are affected. The main types of pelvic organ prolapse include:
Cystocele (Anterior Compartment Prolapse): in cystocele, the bladder bulges into the front wall of the vagina, leading to symptoms such as the sensation of a lump in the vagina, pelvic heaviness/dragging sensation, urinary frequency/urgency, voiding difficulty or hesitancy in initiating a urinary stream, feeling of incomplete emptying (which can translate to high residual urine volumes resulting in increased risk of urinary tract infections and in severe cases, bladder nerve damage and backlog of pressure to the ureters/kidneys causing swelling). Some women may also experience sexual dysfunction, with discomfort during sex or vaginal bleeding in instances of friction with clothing.
Rectocele (Posterior Compartment Prolapse): in cases of rectocele, the rectum bulges into the back wall of the vagina. This can cause symptoms such as a sensation of a lump in the vagina, pelvic heaviness/dragging sensation, and difficulty with bowel movements – in severe cases, some women may need to use their fingers to exert pressure on the back wall of their vagina to be able to defecate properly. Some women may also experience sexual dysfunction, with discomfort during sex or vaginal bleeding in instances of friction with clothing.
Uterine Prolapse (Central Compartment Prolapse):uterine prolapse occurs when the uterus descends into the vaginal space. This can lead to symptoms such as sensation of a lump in the vagina, pelvic heaviness/dragging sensation. Many women may have multiple compartment prolapse, i.e. a cystocele/rectocele and uterine prolapse at the same time.
Vaginal Vault Prolapse: after a hysterectomy, where the uterus is removed, the upper portion/apex of the vagina can sometimes descend or prolapse into the vaginal canal. This is known as vaginal vault prolapse. Symptoms include a feeling of fullness in the vagina or a sensation of something falling out of the vagina.
Enterocele: an enterocele, also known as small bowel prolapse, occurs when the small intestine or peritoneum (the lining of the abdominal cavity) protrudes into the vaginal space – this can sometimes be difficult to diagnose clinically and may simply present as a sensation of a lump in the vagina.
Pelvic organ prolapse can involve various types, each affecting different pelvic organs.
It is important to note that pelvic organ prolapse can involve a combination of these types, and the severity of symptoms and extent of prolapse can vary from person to person – the only way to tell would be via a detailed pelvic examination by a trained urogynaecologist.
Can pelvic organ prolapse be reversed naturally?
Yes, in some cases, mild cases of pelvic organ prolapse (POP) can be reversed/improved without surgery through strategies such as lifestyle changes, pelvic floor exercises, and sometimes the use of supportive devices [10]. While a complete reversal of POP may not always be possible without surgical intervention, these approaches can help in vastly alleviating one’s symptoms, improve pelvic floor strength, and may also help prevent further progression of the condition:
Pelvic floor muscle exercises (Kegels): Kegel exercises can help with pelvic organ prolapse by strengthening the muscles, including the pubococcygeus, iliococcygeus, and puborectalis muscles [11]. These muscles are crucial in maintaining pelvic organ support and preventing prolapse. Regularly contracting and relaxing these muscles can strengthen them over time. Stronger pelvic floor muscles provide better support for the pelvic organs, helping to prevent or alleviate symptoms of pelvic organ prolapse. Over time, one becomes more aware of these muscles and learns how to engage them effectively. This increased awareness can help women better control their pelvic floor muscles, improving bladder and bowel function and reducing symptoms of pelvic organ prolapse. Kegel exercises are often recommended as part of conservative management strategies for pelvic organ prolapse, especially in mild to moderate cases. When combined with lifestyle modifications and other pelvic floor rehabilitation techniques, such as biofeedback or pelvic floor physical therapy, Kegel exercises can be a good non-invasive approach to managing POP and improving pelvic floor function. They are best performed regularly and consistently with the guidance of a healthcare provider or pelvic floor specialist/physiotherapist to maximise their effectiveness and ensure proper technique.
Maintain a healthy weight: excess weight (particularly fat around the abdominal/pelvic region) can strain the pelvic floor muscles and increase the risk of pelvic organ prolapse or worsen it. Maintaining a healthy body weight can help alleviate this pressure, reducing the stress on the pelvic floor and lowering the risk of prolapse. According to the Singapore Heart Foundation, a normal BMI for Asians ranges between 18.5 – 22.9kg/m² [12].
Avoid heavy lifting: activities that involve heavy lifting or straining can exacerbate pelvic organ prolapse by placing increased pressure on the pelvic floor. Try to minimise these activities by using tools to help in daily life, e.g., using a trolley bag instead of carrying heavy bags, avoiding squatting down to do laundry, etc.
Pessaries: a vaginal pessary is a medical device that is inserted into the vagina to help provide mechanical support to the prolapsed pelvic organs. By holding these organs in their anatomical/proper position, pessaries can help alleviate the symptoms of pelvic organ prolapse and aid the pelvic organs in carrying out their normal functions. Pessaries come in various shapes and sizes and need to be fitted by a trained Gynaecologist; once fitted successfully, it can serve as a non-invasive and reversible treatment option for pelvic organ prolapse, particularly for women who may not be suitable candidates for surgery or prefer to avoid surgical intervention. Insertion and removal of vaginal pessaries can be taught to the patient to allow for individualised management of pelvic floor dysfunction, quality of life, and better personal control of one’s life with the resumption of daily activities with greater comfort and confidence, enhancing overall well-being and function.
Healthy diet with regular bowel habits: a balanced diet and regular bowel habits contribute to maintaining a healthy body weight, which reduces the strain on the pelvic floor muscles and supporting structures. A diet rich in fibre, fluids, and nutrients supports regular bowel movements, lowering the risk of constipation. Constipation and straining during bowel movements can put significant pressure on the pelvic floor muscles and increase the risk of pelvic organ prolapse. By promoting regular bowel habits, a healthy diet can help prevent the excessive strain on the pelvic floor and lower the risk of POP.
Stay active: physical activity, particularly exercises that engage the pelvic floor muscles, can strengthen these muscles over time. Strong pelvic floor muscles provide better support for the pelvic organs, reducing the risk of prolapse and alleviating symptoms associated with POP. Regular exercise improves overall muscle tone, including pelvic floor muscles, and is crucial in maintaining a healthy body weight. Staying active also supports bowel regularity by stimulating intestinal contractions and improving digestion.
Pelvic floor muscle exercises, such as Kegels, can help strengthen weakened pelvic floor muscles and reverse pelvic organ prolapse.
However, it is preferable to consult a healthcare provider, such as a gynaecologist, to help manage symptoms and prevent further progression of pelvic organ prolapse.
How is pelvic organ prolapse treated if not reversed naturally?
Pelvic organ prolapse (POP) can be managed through a combination of non-surgical and surgical treatments, depending on the severity of symptoms and individual preferences. Treatment options include:
Medications: in some cases, medications may be prescribed to manage symptoms associated with POP, such as atrophic vaginitis, particularly in postmenopausal women. These can come in the form of topical oestrogen creams/tablets that are administered locally in the vagina and are safe for long-term use in the majority of patients.
Pelvic organ prolapse repair: during pelvic floor repair surgery, the surgeon aims to restore the normal anatomy and support of the pelvic floor by repairing or reinforcing the weakened or damaged pelvic floor muscles and tissues. The specific techniques used in pelvic floor repair surgery may vary depending on the severity and type of prolapse and individual patient factors. The majority of pelvic floor repair surgeries are via the vaginal route, with some utilising abdominal, laparoscopic, or robotic-assisted techniques. The procedure may involve the use of native tissues (or, less commonly, synthetic mesh, e.g. in sacrocolpopexy, where a mesh graft is attached to the top of the vagina and secured to a bony structure in the pelvis called the sacrum, located at the base of the spine to lift the vaginal vault or cervix) to provide additional support to the pelvic organs. Pelvic floor repair surgery is typically performed under general anaesthesia and may be combined with other pelvic reconstructive procedures, such as a hysterectomy if needed. The goal of pelvic floor repair surgery is to alleviate symptoms of pelvic organ prolapse, improve pelvic floor function, and restore quality of life for affected individuals. As with any surgical procedure, pelvic floor repair surgery carries risks and potential complications, and patients should discuss the benefits, risks, and alternatives with their urogynaecologist before undergoing treatment.
Colpocleisis:colpocleisis may be an option in a small select group of women who have failed conservative management but have significant medical comorbidities that make them unsuitable for pelvic floor repair surgeries. Also known as vaginal closure surgery, colpocleisis involves removing a portion of the anterior and posterior vaginal walls and then suturing the remaining vaginal walls together, effectively closing off the vaginal canal. This closure alleviates symptoms of POP by preventing further descent or bulging of the vaginal walls. However, sexual intercourse will not be possible after that, and care should be taken to exclude any potential pelvic malignancies before proceeding with this option.
In conclusion, collaborating with a urogynecologist for individualised management of pelvic organ prolapse (POP) is paramount for optimising patient outcomes and ensuring personalised care. Urogynecologists possess specialised training and expertise in evaluating, diagnosing, and treating pelvic floor disorders, including POP. By working closely with one, patients can benefit from a comprehensive evaluation considering their unique medical history, symptoms, lifestyle factors, and treatment preferences. Furthermore, ongoing communication and collaboration between patients and their urogynecologists facilitate shared decision-making and continuity of individualised care, ultimately leading to improved outcomes, enhanced quality of life, and greater satisfaction with treatment.
References
Michel Bureau, K. V. (2017). Pelvic organ prolapse: A primer for urologists. Canadian Urological Association Journal, doi: 10.5489/cuaj.4634.
Christine Aboseif, P. L. (2022). Pelvic Organ Prolapse. Florida: StatPearls.
Junyan Zhu, J. S. (2023). Association between infant birthweight and pelvic floor muscle strength: a population-based cohort study. BMC Pregnancy and Childbirth.
Juliana Sayuri Kubotani, E. A. (2014). Assessing the Impact of Twin Pregnancies on the Pelvic Floor Using 3-Dimensional Sonography. Journal of Ultrasound in Medicine, https://doi.org/10.7863/ultra.33.7.1179.
Hongmei Zhu, D. Z. (2022). Effect of Pelvic Floor Workout on Pelvic Floor Muscle Function Recovery of Postpartum Women: Protocol for a Randomized Controlled Trial. International Journal of Environmental Research and Public Health, doi: 10.3390/ijerph191711073.
National Institute for Health and Care Excellence (NICE). (2021). Pelvic floor dysfunction: prevention and non-surgical management. London: National Institute for Health and Care Excellence (NICE).
Kari Bø, S. A.-A. (2023). Strenuous physical activity, exercise, and pelvic organ prolapse: a narrative scoping review. International Urogynecology Journal, doi: 10.1007/s00192-023-05450-3.
Lee Una J.a, K. M. (2017). Obesity and pelvic organ prolapse. Current Opinion in Urology, DOI: 10.1097/MOU.0000000000000428.
Andreas Höier Aagesen, N. K. (2023). Hysterectomy on benign indication and risk of pelvic organ prolapse surgery: A national matched cohort study. Acta Obstetricia et Gynecologica Scandinavica, doi: 10.1111/aogs.14561.
Institute for Quality and Efficiency in Health Care (IQWiG). (2021). Pelvic organ prolapse: Pelvic floor exercises and vaginal pessaries. Germany: InformedHealth.org.
Yi-Chen Huang, K.-V. C. (2024). Kegel Exercises. Florida: StatPearls.
This refers to a drooping of the uterus, bladder or rectum beyond the vagina. It is more common in older women. The main cause of this is weakened pelvic floor muscles from damage sustained during pregnancy and childbirth, weakening from ageing and menopause and obesity. Read more about it here.
What is a vaginal pessary?
This is a soft, removable device that is inserted in your vagina to support your prolapsed pelvic organs and hence provide relief of your symptoms of POP. This is temporary as if the pessary is removed, POP will recur. Vaginal pessaries come in many different shapes and sizes. The most commonly used one is the ring pessary, which needs to be removed, washed and replaced by your gynaecologist every 3-4 months or so.
How is a vaginal pessary inserted?
A vaginal pessary can be fitted after a vaginal examination by your gynaecologist in the clinic. Sizing sometimes requires trial and error as every woman’s vagina, degree of prolapse, activity levels and toileting habits are different – much like trying on new shoes! Pessaries that are too small may drop out easily on physical activity or while on the toilet bowl passing urine or motion (particularly if you have a habit of straining). Pessaries that are too large may cause discomfort and rub excessively against the vaginal walls causing ulcerations, bleeding and infection.
What are the advantages of a vaginal pessary?
Relieves the symptoms of POP
Can be fitted in the clinic
Does not interfere with daily activities
Can defer surgery if one is not keen/ ready for it
Does not involve surgical or anaesthesia risks
What are the disadvantages of a vaginal pessary?
Temporary; POP recurs if pessary is removed
Needs regular follow-up for removal, washing and reinsertion
May experience increase in vaginal discharge
Risk of ulceration, bleeding and infection
May interfere with sex (depending on pessary shape). It is possible to have sex as per normal with a ring pessary.
What are the alternatives of a vaginal pessary?
Kegel (pelvic floor) exercises These strengthen and maintain the tone of pelvic floor muscles, which can help to improve the symptoms of POP.
Surgery This is suitable for more severe forms of POP and is a definitive treatment option.
Anything else I need to know?
With menopausal changes causing thin and dry vaginal skin (vaginal atrophy) and the presence of a vaginal pessary, it is important to use topical vaginal estrogen creams and tablets regularly to reduce the risk of ulceration and bleeding.
This refers to a drooping of the uterus, bladder or rectum beyond the vagina. It is more common in older women, affecting 1 in 3 women who have had children. 1 in 10 women will need surgery in their lifetime for POP.
What types of surgery are there for pelvic organ prolapse?
The type of surgery advised by your urogynaecologist will depend on your severity of pelvic organ prolapse, age, general health, medical conditions, surgical history and sexual activity. There is no one-size-fits-all. Each surgery for POP needs to be individualised. Surgery needs to done under general anaesthesia.
Vaginal pelvic reconstructive surgery
This is the most common approach as the pelvic organs are drooping out from the vagina. If the uterus is prolapsed, there is no plans for more children and the woman has no desire to keep her uterus, a vaginal hysterectomy will be performed. The ovaries can be conserved if they are normal.
Surgery for prolapse in the other compartments (pelvic floor repair) involves making a cut in the vagina and separating the prolapsed organ away from the vaginal wall. Stitches or mesh are used to strengthen the defect in the supporting tissue, and the vaginal skin is closed to reduce the bulge.
If this is done for the bladder, it is known as an anterior repair or colporraphy. If this is done for the rectum, it is known as a posterior repair or colporraphy. In some cases, additional permanent sutures may be placed to hitch the top of the vagina to a strong ligament in the pelvis to provide additional support (sacrospinous ligament fixation/SSLF). Overall, there are no cuts on the abdomen.
Risks of surgery include:
Common (affecting 1-5% of patients):
Vaginal bleeding / haematoma – in cases of significant bleeding, blood transfusion and/or additional procedures may be required to stop the bleeding
Postoperative pain (in cases of SSLF, this is usually involves the right buttock and usually resolves in a few weeks)
Urinary retention, infection, frequency, urgency, urge and urinary incontinence
Wound infection
Constipation
Difficulty and/or pain with intercourse
Failure to achieve the desired result; recurrence of prolapse
Earlier onset of menopause
Uncommon (affecting 0.1-1% of patients):
Injury to the bladder
Pelvic abscess
Venous thrombosis (Blood clot in legs) / Pulmonary embolism (Blood clot in lungs)
Rare (affecting <0.1% of patients):
Serious adverse reactions to general anaesthesia
Excessive bleeding requiring transfusion or return to theatre
Injury to the urinary tract / bowel
Admission to the intensive care unit for monitoring should the operation be of prolonged duration or result in complications
Death: the risk is approximately less than 1 in 4000
Mesh usage is typically reserved for the most severe/ recurrent cases due to permanent implantation of synthetic material. This gives a better support for POP compared to stitches, but can only be used by trained urogynaecologists in a select few. There is a risk of mesh complications such as erosion, infection, scarring and chronic pain, which may require further procedures.
Abdominal approach (sacrocolpopexy)
This is an option for women with previous hysterectomy and an apical prolapse (top of vagina collapsing downwards out of the vaginal opening). It involves making cuts in the abdomen and using a permanent synthetic mesh to hitch the vagina up to the sacrum, which is a large triangular bone at the base of the spine.
Vaginal closure surgery
In a few instances, vaginal closure surgery may be recommended for women with severe prolapse who are medically unfit for vaginal pelvic reconstructive surgery and are not sexually active. This surgery involves pushing the prolapsed organs back into the vagina and stitching the vaginal walls together.
How successful is surgical treatment for pelvic organ prolapse?
70% of women will have a long-term cure after undergoing surgery for POP. For those with permanent implantation of synthetic mesh, the success rate goes up to 90%. It is important to note that the limitation of pelvic reconstructive surgery lies in working with ageing/weakened tissues. Hence, pelvic organ prolapse typically recurs due to persistent risk factors that caused the initial prolapse. Although ageing cannot be reversed, lifestyle modifications like maintaining a healthy body mass index (BMI), avoiding chronic cough, constipation and lifting heavy loads remain essential.
The contents on this website provides general information only and does not replace professional or specialist advice. If you think you may have any medical condition, always seek prompt medical attention from a professional healthcare provider. It is not advisable to delay consulting professional advice by relying on the information provided here. Although reasonable efforts have been made to ensure that the information is relevant and comprehensive, we make no guarantees or representation that the contents on this website are complete, up-to-date or accurate. drngkailyn.com is independently owned and is not affiliated or endorsed by any organisation.









{kind=link}