Uterine fibroids are benign (noncancerous) tumours that develop in the uterus and are a common condition affecting a significant proportion of women during their child-bearing, i.e. reproductive years. These growths arise from the muscle layer of the uterus and can vary in size, from as small as a pea to as large as a melon. They may grow singularly or in multiple numbers and can affect different locations of the uterus – the location of fibroids can influence the symptoms a woman experiences as well as the treatment options. Fibroids are known to exhibit slow growth over the years and will usually start shrinking following menopause.
Uterine fibroids are noncancerous uterine growths commonly occurring during a woman’s reproductive years.
How common are uterine fibroids, and who is at the most risk?
Uterine fibroids are quite common, affecting most women by the age of 50 [1]. The prevalence can vary based on age, ethnic background, genetic factors, and lifestyle. They are most commonly diagnosed in women in their 30s and 40s. Factors that increase the risk of developing uterine fibroids include:
Ethnicity:African-American women are more likely to develop fibroids compared to women of other racial and ethnic backgrounds [2].
Family history: there is a higher risk for women who have a family member with fibroids to develop uterine fibroids themselves, as there seems to be a genetic predisposition to this [3].
Lifestyle and environmental factors: although the exact mechanisms of lifestyle and environmental factors that contribute to the risk of developing uterine fibroids are poorly understood, poor diet (e.g., high in red meats and low in fruits/vegetables/fibre) [5], lack of exercise (e.g., sedentary lifestyle) [6], stress [7], alcohol consumption [8], etc., may contribute to the risk of developing fibroids.
Age: fibroids are commonly diagnosed in women between the ages of 30 and 50, although they can develop/occur at any age [9].
Hormonal factors: fibroids tend to grow over the years, with expedited growth during pregnancy [10] (when hormonal levels are high), and occasionally also demonstrate increased growth when one is on hormone replacement therapy (HRT) [11]. Fibroids then commonly shrink over time after a woman attains menopause as hormonal levels decline.
The exact cause of uterine fibroids is still unknown, and the majority of women who have them do not have any of the above risk factors. Regular gynaecological check-ups can help in the early detection and management of uterine fibroids. It is also important to monitor one’s menstrual cycles closely and seek medical attention early should changes be detected.
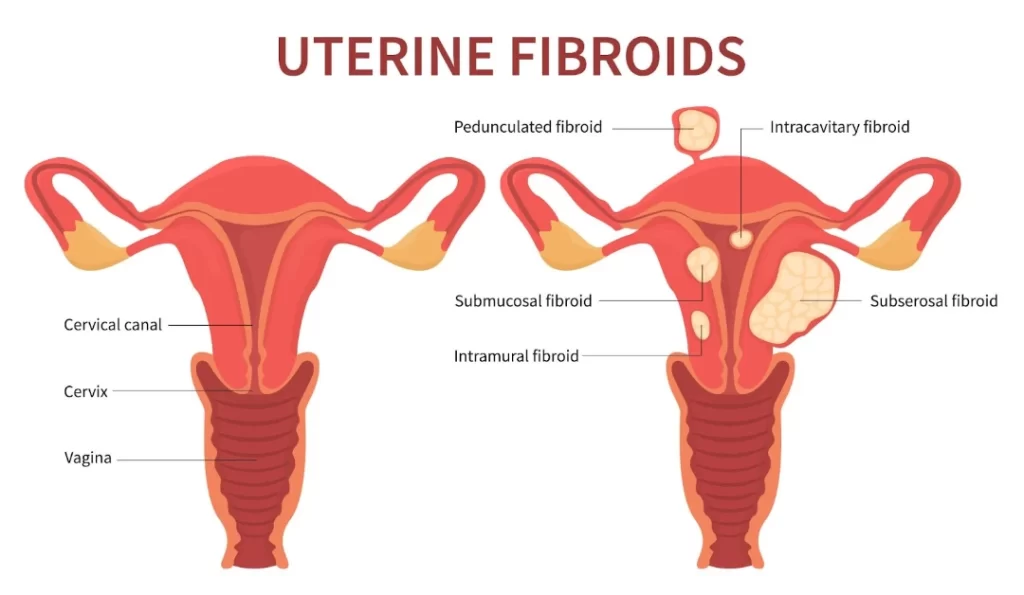
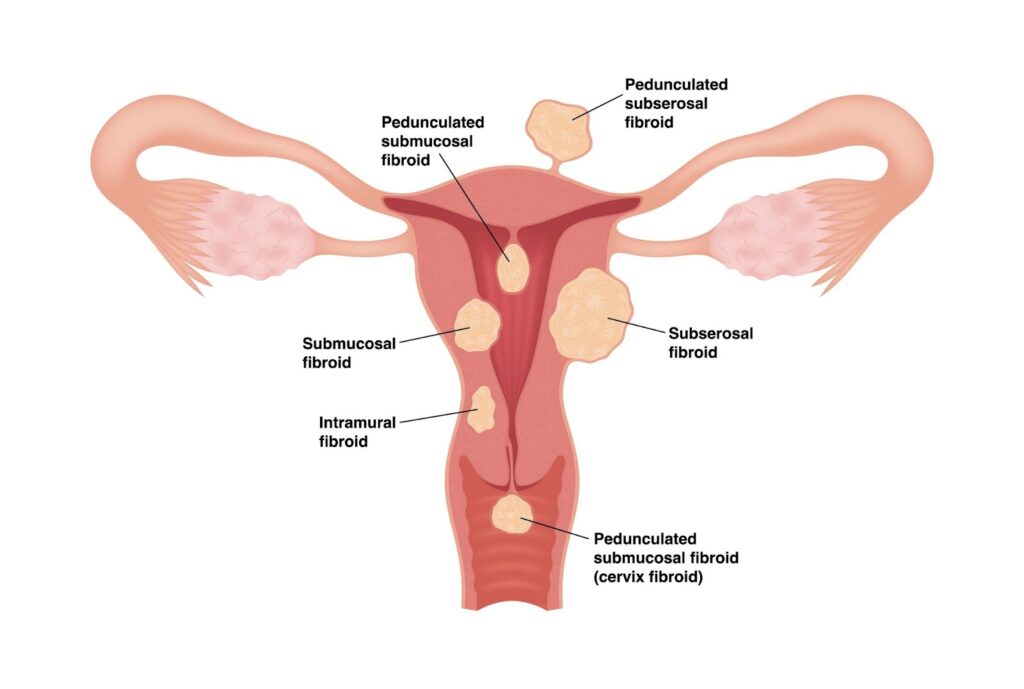
What types of uterine fibroids exist?
Uterine fibroids are generally categorised based on their location within the uterus, leading to different types:
Intramural fibroids are the most common type of fibroids, developing within the muscular wall of the uterus [12]. They can grow larger and cause a larger uterine size than usual, resulting in heavy menstrual bleeding.
Subserosal fibroids: these fibroids grow/develop on the outer serosal layer of the uterus and, depending on their size, can result in extrinsic pressure on surrounding/adjacent organs such as the bladder (leading to urinary frequency, urgency or sensation of incomplete emptying) or the rectum (leading to constipation), or simply pelvic heaviness or a palpable pelvic-abdominal mass [13]. They may be connected to the uterus by a narrow stalk, which is why they are called pedunculated fibroids.
Submucosal fibroids: less common than the other types, these fibroids develop in the submucosal layer (the innermost layer) of the uterus [14]. They can protrude into the uterine cavity, leading to heavy/prolonged/frequent/unscheduled menstrual bleeding as well as fertility issues.
Pedunculated fibroids:pedunculated fibroids grow on a stalk either inside the uterine cavity (pedunculated submucosal) or on the outer surface of the uterus (pedunculated subserosal) [15]. They can sometimes twist, causing severe pain and necessitating emergency treatment.
Cervical fibroids:cervical fibroids occur in the cervix, the lower part of the uterus, and are relatively rare compared to the other types [16].
Uterine fibroids are categorised into different types based on their location.
The location and size of the fibroids significantly influence the symptoms they may cause and the treatment options available. Some fibroids involve more than one location, i.e. transmural and may be challenging to treat.
Are uterine fibroids benign or malignant?
Uterine fibroids are benign, which means they are noncancerous growths. They originate from the muscle tissue of the uterus, and while they can vary in size and number, they do not spread to other parts of the body as malignant (cancerous) tumours would.
Although fibroids are not associated with an increased risk of uterine cancer and are almost always benign (over 99% of fibroids are benign), they can still cause significant health issues, including menstrual disturbances such as heavy menstrual bleeding, pelvic pain, and pressure symptoms affecting the bladder or rectum. However, a small proportion of fibroids may rarely undergo malignant transformation to become cancerous – these usually present with rapidly enlarging size of fibroids and are termed leiomyosarcoma [17].
How can uterine fibroids be distinguished from uterine cancer?
Uterine fibroids and uterine cancer, such as endometrial cancer or leiomyosarcoma, can have different symptoms and characteristics. Fibroids often cause symptoms like abnormal uterine bleeding. At the same time, uterine cancer may present with similar symptoms. Still, it may also include rapidly enlarging the size of fibroids and other constitutional symptoms such as loss of appetite, weight loss, etc.
To differentiate between fibroids and cancer, the following diagnostic methods are commonly used:
Ultrasound: a pelvic ultrasound is often the first step in evaluating the presence of fibroids and can help distinguish them from other types of growths.
Magnetic resonance imaging (MRI): an MRI can provide detailed images of the uterus, helping to identify the nature of the growths and distinguish between benign fibroids and potential malignancies.
Endometrial biopsy: an endometrial biopsy involves obtaining a sample of the endometrium (the lining of the uterus) and examining it for abnormal cells. This can help diagnose uterine cancer.
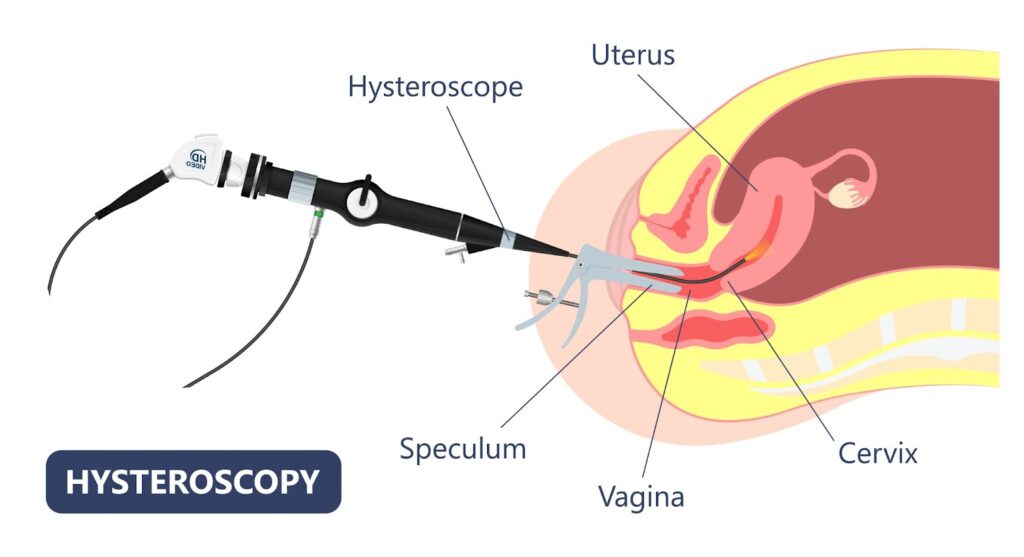
Hysteroscopy: a hysteroscopy is a procedure where a small camera is inserted into the uterus to directly visualise the uterine cavity, which can help identify abnormal growths and allow for biopsy.
It is through a combination of these diagnostic methods, along with a thorough medical history and examination, that doctors can differentiate between uterine fibroids and cancer.
A hysteroscopy involves inserting a small camera into the uterus to visualise the uterine canal.
How are uterine fibroids managed and treated?
Uterine fibroids can be managed and treated using various approaches, depending on the size and location of the fibroids, the severity of symptoms, the woman’s age, and her desire for future pregnancies. Treatment options range from watchful waiting to medication and surgery:
Watchful waiting: many fibroids are asymptomatic and do not require immediate treatment. In these cases, regular monitoring of the fibroid’s size and symptoms may be all that is needed.
Medications
Nonsteroidal anti-inflammatory drugs (NSAIDs):NSAIDs can be used to relieve menstrual cramps, which may be associated with fibroids; however, they only serve as symptomatic relief and do not reduce fibroid size.
Tranexamic acid tablets: these are oral fibrinolytic tablets that can help alleviate heavy menstrual flow and clot passage; however, they only serve as symptomatic relief and do not reduce fibroid size.
Oral contraceptive pills: thesecan help alleviate both heavy menstrual bleeding and cramps and also provide other functions such as menstrual regulation and birth control; however, they do not reduce fibroid size.
Levonorgestrel intrauterine device (IUD):IUD can be effective in reducing heavy menstrual bleeding and cramps caused by fibroids [18]; however, they can only be inserted in selected cases where the uterus is not too enlarged from fibroids, and there are no submucosal fibroids present that distort the endometrial cavity. It is also able to provide contraception at the same time.
Hormonal injection: medications like gonadotropin-releasing hormone (GnRH) agonists (usually administered via intramuscular injections) can shrink fibroids by reducing oestrogen and progesterone levels, but they are typically used only short-term due to potential side effects such as hot flushes, mood swings, bone mineral density loss, etc. There is also a risk of rebound fibroid growth following cessation of GnRH therapy. They are, hence, sometimes given as an adjuvant preoperative measure in an attempt to temporarily shrink fibroids before going in for definitive surgical management.
Non-surgical procedures
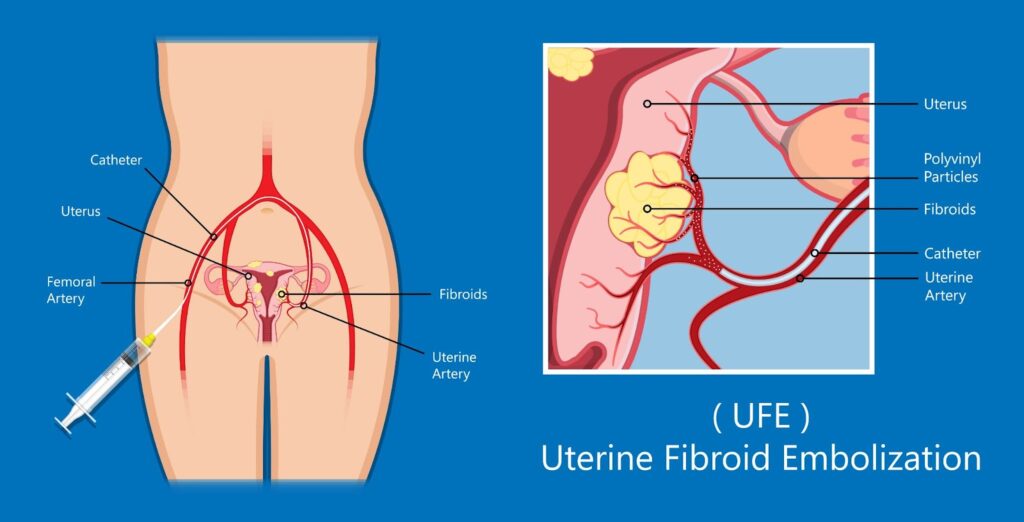
Uterine artery embolisation (UAE): a minimally invasive procedure where small particles are injected into the arteries supplying the fibroids, cutting off their blood supply and causing them to shrink. An interventional radiologist usually does this as a day surgery procedure and may require sedation. Women typically experience good short-term relief of their symptoms as their fibroids shrink (different fibroid locations may respond differently to UAE); however, due to a significant risk of fibroid regrowth with a lack of long-term efficacy, there is a significant proportion of women who will require downstream repeated treatment(s) and ultimately end up in definitive surgical management.
High-intensity focused ultrasound/MRI-guided focused ultrasound surgery (HIFU/MRgFUS): HIFU/MRgFUS uses high-frequency ultrasound sound waves to heat fibroid tissue, with the heat resulting in destruction/ablation of the targeted fibroid tissue; however, only certain fibroid locations are more amenable to this treatment modality as there is a risk of inadvertent injury to surrounding organs otherwise. Again, whilst this is a minimally invasive option and women typically experience good short-term relief of their symptoms as their fibroids shrink, due to a significant risk of fibroid regrowth with a lack of long-term efficacy, there is a significant proportion of women who will require downstream repeated treatment(s) and ultimately end up in definitive surgical management.
Uterine fibroid embolisation/uterine artery embolisation is a minimally invasive procedure that cuts off fibroids’ blood supply.
Surgical options
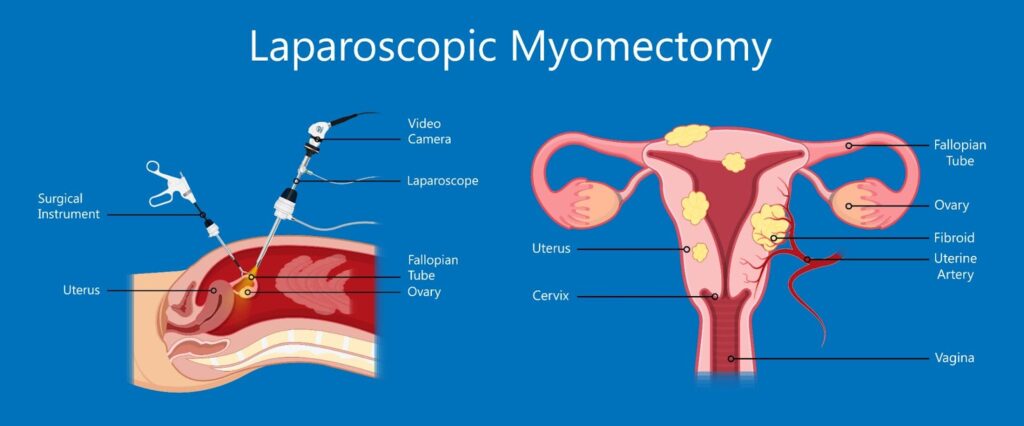
Myomectomy:myomectomy is the surgical removal of fibroids while leaving the uterus in place. This is typically the preferred surgical option for women still desiring fertility or preferring uterine conservation. Myomectomy can be done either via the open/laparotomy approach or, more commonly, through the laparoscopic approach – the best surgical approach is usually individualised. It depends on variables such as the size, number, and location of fibroids/uterus. However, myomectomy is associated with an increased risk of haemorrhage (intra-operative blood loss) as well as fibroid recurrence compared to a hysterectomy (see below); one is typically also advised to avoid conceiving within 6-12 months of a myomectomy to reduce risk of pregnancy complications. Women with previous myomectomies may sometimes be advised to consider caesarean sections as their future mode of delivery, depending on the size and location of fibroids removed.
Transcervical (hysteroscopic) resection of myoma: this treatment modality is specifically for submucous fibroids, where a hysteroscopy is introduced through the vaginal canal via the cervical canal into the uterine cavity. A resectoscope is typically used to cut the submucous fibroid into smaller chips, which are, in turn, removed from the uterus vaginally. This procedure is generally performed as a day surgery.
Hysterectomy: a hysterectomy is the complete surgical removal of the uterus. This is considered a definitive treatment for fibroids (with no future risk of fibroid recurrence) and is suitable for women who have completed their family and are no longer desiring fertility. Following a hysterectomy, one will no longer have periods nor have the ability to carry pregnancies. A hysterectomy may be done either via the open/laparotomy approach or, more commonly, through the laparoscopic approach. The best surgical approach is usually individualised and depends on different variables, such as the size and mobility of the uterus. It is commonly done in conjunction with bilateral salpingectomy (removal of both fallopian tubes, as the tubes are attached to the uterus). Depending on age and preferences, ovaries can be conserved during a hysterectomy. If the ovaries are conserved, one will continue to have normal levels of female hormones and will not be deemed menopausal (even if there are no longer periods). If the ovaries are removed at the same setting as a hysterectomy, then one will be considered to be surgically menopausal.
Laparoscopic myomectomy is a minimally invasive surgical procedure used to remove uterine fibroids through small incisions, resulting in less pain and a quicker recovery.
Lifestyle and alternative treatments
Diet and exercise:evidence suggests that maintaining a healthy weight and following a diet low in red meat and high in green vegetables may help manage symptoms [19].
Alternative medicine: acupuncture, herbal remedies, and yoga may provide symptom relief for some women, but more research is needed to confirm their efficacy.
It is important to note that whilst lifestyle and alternative treatments can help alleviate symptoms arising from uterine fibroids, they do not shrink fibroids or make them disappear. The choice of definitive treatment depends on various factors, and a gynaecologist can recommend the best option based on the individual’s condition and preferences. Regular follow-ups are important to monitor the fibroids and adjust treatment as necessary.
References
Anne Zimmermann, D. B. (2012). Prevalence, symptoms and management of uterine fibroids: an international internet-based survey of 21,746 women. BMC Women’s Health, doi: 10.1186/1472-6874-12-6.
Elizabeth A. Stewart, W. K. (2013). The Burden of Uterine Fibroids for African-American Women: Results of a National Survey. Journal of Women’s Health, doi: 10.1089/jwh.2013.4334.
Veronica Medikare, L. R. (2011). The Genetic Bases of Uterine Fibroids; A Review. Journal of Reproduction and Infertility, 181-191.
Qiwei Yang, M. C. (2022). Comprehensive Review of Uterine Fibroids: Developmental Origin, Pathogenesis, and Treatment. Endocrine Reviews, doi: 10.1210/endrev/bnab039.
Andrea Tinelli, M. V. (2021). Uterine Fibroids and Diet. International Journal of Environmental Research and Public Health, doi: 10.3390/ijerph18031066.
Yunrui Sun, X. H. (2023). Association between leisure sedentary behaviour and uterine fibroids in non-menopausal women: a population-based study. BMJ Open, doi: 10.1136/bmjopen-2023-073592.
Anissa I. VINES, M. T. (2011). The Association between Self-Reported Major Life Events and the Presence of Uterine Fibroids. Women’s Health Issues, doi: 10.1016/j.whi.2010.03.009.
Hajra Takala, Q. Y.-H. (2020). Alcohol Consumption and Risk of Uterine Fibroids. Current Molecular Medicine, doi: 10.2174/1566524019666191014170912.
Zheng Lou, Y. H. (2023). Global, regional, and national time trends in incidence, prevalence, years lived with disability for uterine fibroids, 1990–2019: an age-period-cohort analysis for the global burden of disease 2019 study. BMC Public Health.
Mihaela Camelia Tîrnovanu, L. L. (2022). Uterine Fibroids and Pregnancy: A Review of the Challenges from a Romanian Tertiary Level Institution. Healthcare (Basel), doi: 10.3390/healthcare10050855.
Elisa Moro, E. D. (2019). The Impact of Hormonal Replacement Treatment in Postmenopausal Women with Uterine Fibroids: A State-of-the-Art Review of the Literature. Medicina (Kaunas), doi: 10.3390/medicina55090549.
Wojciech Wrona, A. S. (2017). The role of levonorgestrel intrauterine systems in the treatment of symptomatic fibroids. Menopause Review, doi: 10.5114/pm.2017.72758.
The menstrual cycle, also known as menstruation or periods in Singapore, occurs when there is shedding of the uterus lining (otherwise known as the endometrial lining) – which comprises blood and tissue. It helps the body prepare for pregnancy and typically starts at puberty and ends in menopause; this is when menstruation stops for an entire year [1].
Menstrual cycles begin at puberty and end at menopause.
The menstrual cycle takes place as a result of hormones and has three phases:
Follicular phase: this refers to the first half of the menstrual cycle and starts from Day 1 of your period, lasting until ovulation. The first few days (lasting up to a week) are characterised by the shedding of the uterine lining, which women recognise as their period blood. The ovaries then start developing a few follicles (each containing an immature egg), with one becoming the dominant one, which continues to mature. This phase is also characterised by endometrial proliferation [2], whereby oestrogen stimulates the thickening of the uterine lining in preparation for potential embryo implantation should the woman fall pregnant.
Ovulation phase: ovulation typically occurs mid-cycle, e.g. in a 28-day cycle. It usually occurs around day 14 but varies depending on the cycle. During ovulation, the mature egg is released from the dominant follicle, and this egg is picked up by the fimbrial end of the fallopian tube, where it waits to meet a sperm.
Luteal phase: following ovulation, the luteal phase starts – marking the second half of the menstrual cycle. The follicle that releases the egg forms a corpus luteum, which begins secreting progesterone to stabilise the uterine lining to prepare for a potential pregnancy. If there is no pregnancy, the uterine lining sheds, and the next period occurs.
How long is a normal menstrual cycle?
A normal menstrual cycle varies between individuals in Singapore, but the average length is usually 28 days. However, a normal interval between periods (from Day 1 of one period to Day 1 of the next period) is defined as anywhere between 21 to 35 days [3]. It is also important to remember that the number of days between each period will vary between women, even within the same individual. Various things can cause the length of your menstrual cycle to change; these include:
Stress: high stress levels can result in hormonal disruption, resulting in disturbances in ovulation [4]. Anovulation is when the ovaries do not release an egg during the menstrual cycle, resulting in shorter/longer cycles or irregular periods. In extreme circumstances, this can even lead to secondary amenorrhoea, defined as the absence of menstruation in a person who previously had periods [5]. Other ways that stress can impact menstruation include increased cramps, bloatedness, and mood swings related to periods.
Sickness: sickness or illness can affect one’s menstrual cycle, although the extent and impact depends on the specific illness, its severity and the individual’s overall health [6]. Certain conditions can result in hormonal disruptions and affect the regularity of ovulation, resulting in menstrual disturbances.
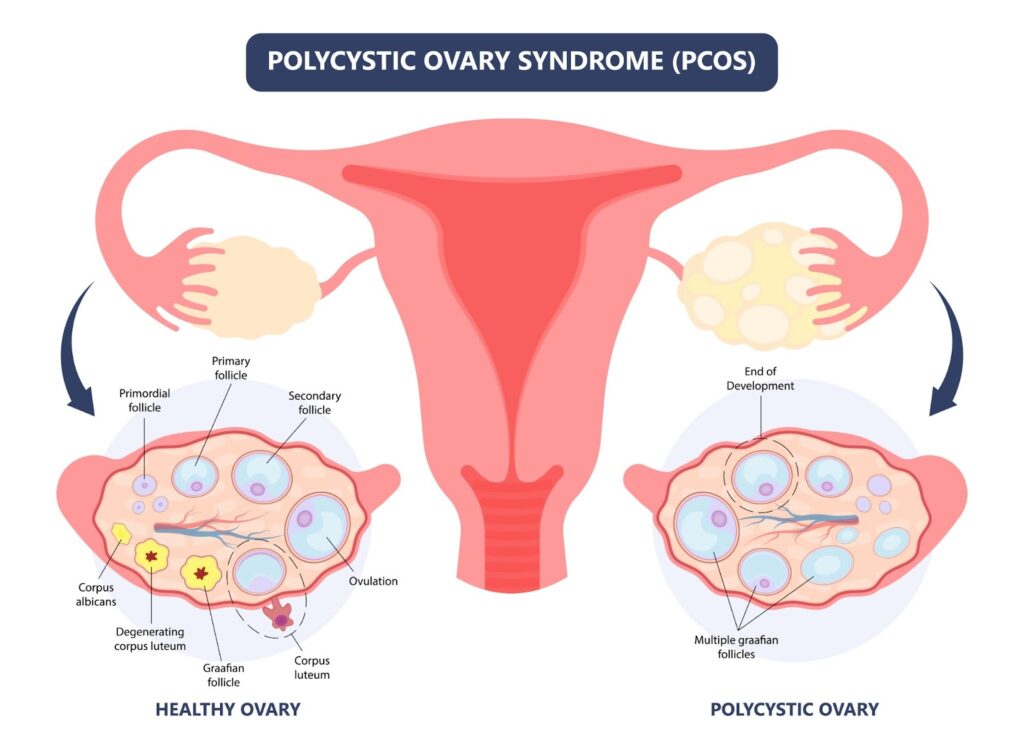
Hormones: hormones outside the reproductive sphere can also cause disruptions in one’s menstrual cycle [7]. Most commonly, thyroid disorders such as hypothyroidism or hyperthyroidism can manifest in irregular periods or erratic menstrual bleeding. Hormonal imbalances within the reproductive sphere can also result in menstrual disturbances, commonly PCOS (polycystic ovary syndrome), where there is hyperandrogenism (increased levels of testosterone) that typically presents with abnormal menstrual patterns. Natural hormonal fluctuations can also occur in the pubertal and peri-menopausal transition phases.
Lifestyle: significant weight changes, particularly within a relatively short period of time (both involving weight loss or weight gain), can affect hormonal balances and, hence, menstrual irregularity [8]. Women with eating disorders, obesity or exercising excessively are all susceptible to menstrual disturbances.
Medications: some medications, including hormonal contraception (oral/implants), psychotropic medications, etc, can influence one’s menstrual patterns, and it is important to discuss with your gynaecologist before starting on these.
Structural issues: things that affect the structural integrity of the female reproductive organs, namely endometrial polyps, uterine fibroids, ovarian cysts, etc, can impact one’s menstrual cycles.
Pregnancy and breastfeeding: pregnancy results in a temporary cessation of menstruation, and breastfeeding following childbirth typically results in a delay in the resumption of normal periods.
For most women, a typical period/menstruation usually lasts no more than seven days.
Breastfeeding following childbirth usually results in a delay in the resumption of normal periods.
What are the common symptoms of menstruation in Singapore?
In addition to bleeding, the other symptoms associated with menstruation include:
Cramping: menstrual cramps, otherwise known as dysmenorrhoea, are commonly experienced amongst women and result from the uterus contracting to expel its lining. Some women perceive more menstrual cramps than others and are usually able to manage them with conservative measures such as heat packs, simple analgesia, etc.
Mood swings: some women may experience irritability, mood swings or changes in their emotional state, more commonly in the lead-up to their menstruation due to hormonal fluctuations. If it is cyclical and affects your ability to function, it may be part of PMS (pre-menstrual syndrome).
Bodily symptoms such as breast tenderness/abdominal bloatedness: hormonal fluctuations can also lead to breast tenderness/sensitivity in the lead-up to menstruation, with a sensation of abdominal bloatedness/water retention. Some women may also experience fatigue, headaches, or appetite changes.
Changes in vaginal discharge: some women may notice changes in colour and consistency of their vaginal discharge depending on the phase of their menstrual cycles; immediately before and after ovulation, the cervical mucus/vaginal discharge may appear more clear and slippery, whilst, after ovulation, it typically changes to a more sticky texture.
Mild cramping during menstruation is normal as the uterus sheds its lining.
What is an irregular period?
An irregular period is when the gap between each menstrual cycle is less than 21 days or more than 35 days. There are also other characteristics of abnormal periods; these are:
Menstrual flow: periods that are lighter or heavier (requiring frequent pad changes) than normal are signs of an abnormal period. If you find yourself changing your pad on an hourly basis, passing a fair number of sizable clots, flooding your pad in a relatively short time, or having frequent “accidents” of staining your underwear/pants/chairs, then you should seek a gynaecologist’s opinion.
Length of menstrual cycle: for intervals longer than the typical 21-35 days, it is referred to as oligomenorrhoea. Women with this usually experience irregular periods that occur less frequently than normal. The most common cause of this is PCOS (polycystic ovary syndrome), where there is an issue with hormonal imbalances and hence ovulation [9]. On the other end of the spectrum, polymenorrhoea is a menstrual cycle characterised by abnormally short intervals between periods, i.e. shorter than 21 days. This typically results in a woman experiencing periods that occur more frequently than normal.
Missing periods: missing periods, also known as amenorrhoea, can be subdivided into primary and secondary amenorrhoea. Primary amenorrhoea refers to the absence of menstrual periods in a young adolescent who has yet to experience her first menstruation, usually by the age of 16 [10]. Secondary amenorrhoea refers to the absence of menstrual periods in a woman who previously experienced periods – the most common reason being pregnancy, but also hormonal disorders like PCOS [5].
Prolonged periods: periods lasting beyond seven days are defined as prolonged and usually result from hormonal imbalances, structural issues such as uterine fibroids, endometrial polyps, ovarian cysts, blood clotting disorders, use of medications (such as anticoagulants or hormonal medications) or contraceptive implants, or underlying medical conditions.
Unscheduled vaginal bleeding: this is either known as intermenstrual bleeding (IMB), which refers to unscheduled bleeding that occurs in between menstrual cycles, or post-coital bleeding (PCB), which refers to unexpected bleeding following sexual intercourse.
Severe pain or nausea: if you experience bad menstrual cramps, i.e. dysmenorrhoea (this may occur in your lower abdomen/pelvis or radiate to the lower back/thighs) that affects your ability to function and quality of life, it is advisable to see a gynaecologist for further evaluation as you may have gynaecological conditions such as endometriosis, adenomyosis, uterine fibroids, endometrial polyps, pelvic inflammatory disease (PID), etc.
Ascending infection from the vagina upwards towards the uterus, fallopian tubes, and ovaries
Primary ovarian insufficiency
Irregular periods, oligomenorrhoea, period flow getting lighter and lasting for a shorter duration. May also be accompanied by vasomotor symptoms such as hot flushes, mood swings, insomnia, body aches, etc.
Loss of ovarian function before the age of 40, previously known as premature ovarian failure or early menopause
Uterine or cervical cancer
Unscheduled bleeding, heavy menstrual flow, abnormal vaginal discharge
Certain conditions may increase the risk of uterine/cervical cancer, including PCOS, obesity, HPV infection, etc.
Polycystic Ovary Syndrome (PCOS) is characterised by irregular periods, weight gain, acne, and hair loss.
Can you get pregnant with irregular periods?
While it may be challenging to get pregnant if you have irregular periods, it is not impossible. Here are some ways to increase your chances of conceiving:
Have regular sex: having higher sex frequency (every 2-3 days throughout the month) will increase your chances of conceiving naturally since you may be having irregular periods due to erratic ovulation.
Tracking your ovulation: this can be done in various ways, including ovulation tracking apps, urine ovulation test kits, blood tests, or even ultrasound scans. Tracking your ovulation and timing your sexual intercourse in accordance with that will increase your chances of getting pregnant.
Having a healthy lifestyle: this includes adopting a healthy diet, exercising regularly, reducing stress, getting adequate rest, and avoiding smoking/drugs/excessive alcoholic or caffeinated beverages.
Getting a fertility screen: your gynaecologist will be able to go through the various tests/investigations required for you and your partner to understand your fertility health and suggest potential solutions depending on the uncovered issues. If you are over 35, doing this sooner rather than later is advisable.
Is there a way to make an irregular period regular?
This depends on what is causing your irregular periods. If it is caused by certain lifestyle factors such as stress, unhealthy diet, or temporary medications/sickness, your periods can become regular again once these lifestyle factors are back to the status quo.
However, if your irregular periods are caused by medical conditions such as PCOS, you will need to discuss with your gynaecologist the appropriate management options, which should be tailored to your specific circumstances, e.g. fertility desires, timeline, etc and individualised accordingly.
With the help of your gynaecologist, you, too, can live a fulfilled life with irregular periods.
Tetrokalashvili., C. N. (2022). Menstrual Cycle Proliferative And Follicular Phase. Florida: Stat Pearls.
Carr, B. G. (2018). The Normal Menstrual Cycle and the Control of Ovulation. South Dartmouth: Endotext.
Pilar Vigil, c. a. (2022). Chronic Stress and Ovulatory Dysfunction: Implications in Times of COVID-19. Frontiers in Global Women’s Health, doi: 10.3389/fgwh.2022.866104.
Lord, M., & Sahni, M. (2022). Secondary Amenorrhea. Florida: Stat Pearls.
Thiyagarajan, D. K., Basit, H., & Jeanmonod, R. (2022). Physiology, Menstrual Cycle. Florida: Stat Pearls.
Shrinjana Dhar, K. K. (2023). Influence of lifestyle factors with the outcome of menstrual disorders among adolescents and young women in West Bengal, India. Scientific Reports.
Riaz, Y., & Parekh, U. (2023). Oligomenorrhea. Florida: Stat Pearls.
Gasner, A., & Rehman, A. (2023). Primary Amenorrhea. Florida: Stat Pearls.
Urinary incontinence (UI) is a common condition affecting millions of men and women worldwide, and occurs when one leaks urine involuntarily.
There are several types of urinary incontinence, namely:
1. Stress Urinary Incontinence (SUI): where one leaks urine involuntarily during physical activity i.e. on coughing, sneezing, jumping, laughing or exercising.
2.Urge urinary incontinence (UUI): when one leaks urine involuntarily shortly after experiencing a strong urge to urinate, i.e. not able to make it to the toilet in time after the feeling of needing to urinate hits you.
3. Mixed urinary incontinence (MUI): where one leaks urine involuntarily under both the fore-mentioned circumstances.
4. Overflow urinary incontinence: where one leaks or dribbles urine involuntarily (and without sensation) when the bladder is too full/overdistended.
What causes urinary incontinence in women?
The major causes of female urinary incontinence include:
Weakened pelvic floor muscles
A woman’s pelvic floor muscles form the base of the pelvis and work like a hammock to support the pelvic organs, which include the bladder, uterus (womb) and rectum. Risk factors that damage a woman’s pelvic floor includes;
– Damage sustained from pregnancy and childbirth
– Chronic stress on the pelvic floor muscles from obesity
– Chronic cough/constipation
– Lifting of heavy loads
– Ageing
– Menopause
Weakened bladder muscles
Aging results in degeneration and nerve damage, resulting in urinary incontinence.
Urinary Tract Infections (UTIs)
These can result in painful urination, foul-smelling urine, urinary frequency and urgency and UI as well. These symptoms typically resolve after treatment of UTI.
Other things that can worsen female urinary incontinence include:
– Drinking caffeine e.g. tea, coffee and alcohol
– Medical conditions such as poorly controlled asthma, chronic cough, suboptimal diabetic control
– Smoking
What causes urinary incontinence in men?
Majority of male urinary incontinence revolves around:
Prostate problems
As a man’s prostate gets enlarged, this leads to urinary symptoms such as frequent urination, weak stream and UI. In cases where the prostate is resected e.g. for cancer, SUI may occur as a result in men as well.
Nerve damage
Neurological conditions like Parkinson’s disease, stroke, diabetes, spinal cord disease, dementia can cause male UI. Surgery to the lower back or major bowel surgery can sometimes also cause nerve damage that manifests in UI.
Urinary Tract Infections (UTIs)
Similar to women, urinary tract infections can result in painful urination, foul-smelling urine, urinary frequency and urgency and urinary incontinence as well. These symptoms typically resolve after treatment of UTI.
Factors that aggravate urinary incontinence in women can also do the same for men.
Is urinary incontinence more common in women or men, and why?
The prevalence of UI in men is much lower than in women, about 3-11% overall, with UUI accounting for 40-80% of all male patients. SUI takes up less than 10%[1] of male cases and is usually due to prostate surgery, trauma or neurological injury.
Urinary incontinence remains a big problem in women – a local study[2] looking at 1119 healthy Singaporean mid-life women aged 45-69 years revealed that over 1 in 2 reported the presence of any UI, with MUI and SUI each affecting 20% of women – and these were statistics in women who were not actively seeking medical attention for their urinary incontinence, which tells you the dismal awareness of both patients and healthcare professionals about this major morbidity.
The main reason why the prevalence of urinary incontinence is so different between men and women is because our urinary tracts are built very differently in terms of anatomy, and women go through significant life events such as pregnancy and childbirth that men do not – it is hard being a woman indeed!
How does urinary incontinence differ between men and women?
In general, SUI is more commonly experienced by women as opposed to men due to damage sustained from pregnancy and childbirth; whilst if men are affected by urinary incontinence, it is more likely to be that of urge urinary incontinence.
Women are also much more prone to getting UTIs compared to men, as their urethra (urine pipe that transmits urine from the bladder to the urinary meatus i.e. external opening of the body) is considerably shorter due to the absence of penile length – a local study published in the Singapore Medical Journal[3] showed that adult women are 30 times more likely than men to develop UTI.
Conversely in men, the prostate can play a confounding role in the presentation of urinary symptoms in men, where enlargement can result in bladder outlet obstruction (BOO) – rare in women – and manifest in overactive bladder.
Once either gender starts experiencing symptoms of urinary incontinence, however, the severity and impact on one’s quality of life remains the same.
Someone suffering from urinary incontinence may face difficulty in maintaining perineal hygiene, find that their lives revolve around the (nearest) toilet, or feel embarrassment from the perennial “urine” smell emulating from down below with the potential need of wearing adult pads or diapers to avoid “accidents” – over time, this can have a significant impact on one’s ability to go about their daily lives normally, greatly reduce one’s self-esteem and body perception, and even adversely affect interpersonal relationships and sex life.
Are treatment options the same?
Treatment options of urinary incontinence depend more on the cause of incontinence rather than being gender specific, e.g. antibiotic treatment in cases of urinary tract infections (UTIs), or anticholinergic medications/behavioral therapy in cases of overactive bladder and/or UUI.
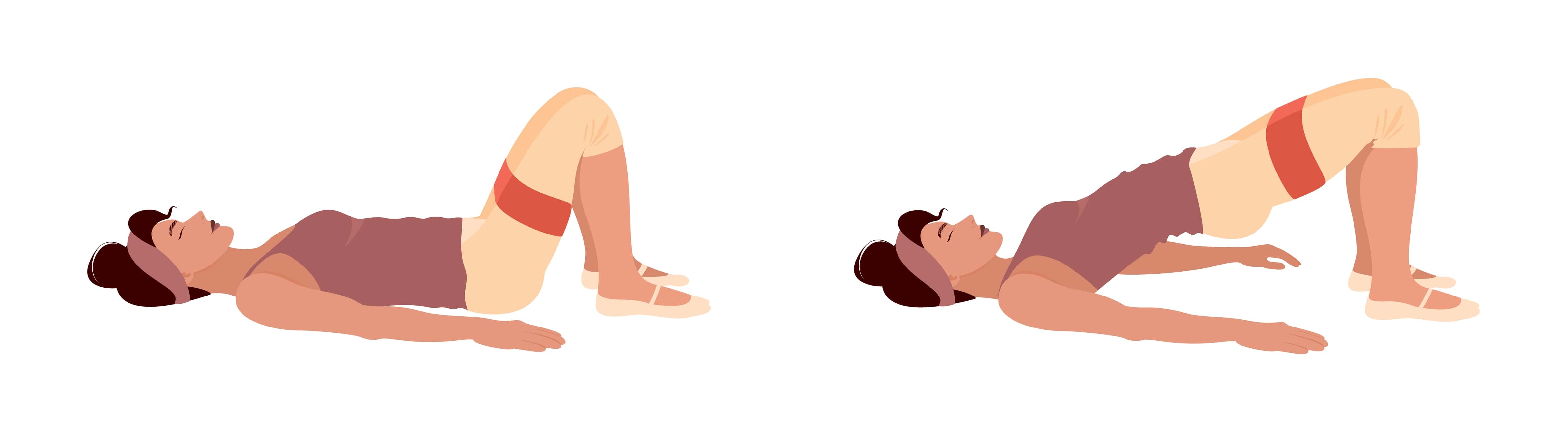
In cases of weakened pelvic floor muscles for example, the mainstay of treatment involves Kegels (pelvic floor) exercises, which can be taught bedside and reinforced with aid from a trained physiotherapist.
The aim and function of Kegels exercises are to strengthen the bulk and tone of one’s pelvic floor and alleviate the symptoms of SUI; to a certain extent, it can also help as part of bladder training for overactive bladder and UUI.
For female SUI that remain refractory to Kegels exercises, surgical intervention such as a mid-urethral sling or colposuspension may be considered.
Lifestyle modifications to reduce or avoid factors that aggravate the symptoms of urinary incontinence can be helpful in both genders – this includes;
– Reduction in caffeine/alcohol intake
– Smoking cessation
– Optimisation of body mass index via adoption of a healthy diet/exercise regimen
In cases where the prostate is contributory to urinary incontinence, a urologist’s input may be required to address this. Neurological disorders resulting in urinary incontinence can be complex to manage and a multi-disciplinary approach needs to be taken to optimize control of the relevant medical condition.
Conclusion
All in all, treatment options need to:
1. Be tailored to the individual
2. Target the predominant complaint/ symptoms that causes the most bother, i.e. if one suffers from MUI but experiences bothersome UUI more often than SUI, the stepwise approach is generally to target the symptoms of UUI first and foremost.
A simple and objective way that one can use at home to track one’s progress in the management of urinary incontinence would be via a bladder diary, which is a self-assessment tool that allows one to record how much and when they drink fluids, as well as how much and when they void, including episodes of urinary incontinence, if any.
An example of that can be found here, and will serve as a helpful adjunct to monitoring treatment for both the patient as well as the healthcare professional.
References
1. Nitti V. W. (2001). The prevalence of urinary incontinence. Reviews in urology, 3 Suppl 1(Suppl 1), S2–S6.
2. Ng, K. L., Ng, K., Thu, W., Kramer, M. S., Logan, S., & Yong, E. L. (2020). Risk factors and prevalence of urinary incontinence in mid-life Singaporean women: the Integrated Women’s Health Program. International urogynecology journal, 31(9), 1829–1837. https://doi.org/10.1007/s00192-019-04132-3
3. http://www.smj.org.sg/article/urinary-tract-infections-adults
What is pelvic organ prolapse (POP)?
This refers to a drooping of the uterus, bladder or rectum beyond the vagina. It is more common in older women. The main cause of this is weakened pelvic floor muscles from damage sustained during pregnancy and childbirth, weakening from ageing and menopause and obesity. Read more about it here.
What is a vaginal pessary?
This is a soft, removable device that is inserted in your vagina to support your prolapsed pelvic organs and hence provide relief of your symptoms of POP. This is temporary as if the pessary is removed, POP will recur. Vaginal pessaries come in many different shapes and sizes. The most commonly used one is the ring pessary, which needs to be removed, washed and replaced by your gynaecologist every 3-4 months or so.
How is a vaginal pessary inserted?
A vaginal pessary can be fitted after a vaginal examination by your gynaecologist in the clinic. Sizing sometimes requires trial and error as every woman’s vagina, degree of prolapse, activity levels and toileting habits are different – much like trying on new shoes! Pessaries that are too small may drop out easily on physical activity or while on the toilet bowl passing urine or motion (particularly if you have a habit of straining). Pessaries that are too large may cause discomfort and rub excessively against the vaginal walls causing ulcerations, bleeding and infection.
What are the advantages of a vaginal pessary?
Relieves the symptoms of POP
Can be fitted in the clinic
Does not interfere with daily activities
Can defer surgery if one is not keen/ ready for it
Does not involve surgical or anaesthesia risks
What are the disadvantages of a vaginal pessary?
Temporary; POP recurs if pessary is removed
Needs regular follow-up for removal, washing and reinsertion
May experience increase in vaginal discharge
Risk of ulceration, bleeding and infection
May interfere with sex (depending on pessary shape). It is possible to have sex as per normal with a ring pessary.
What are the alternatives of a vaginal pessary?
Kegel (pelvic floor) exercises These strengthen and maintain the tone of pelvic floor muscles, which can help to improve the symptoms of POP.
Surgery This is suitable for more severe forms of POP and is a definitive treatment option.
Anything else I need to know?
With menopausal changes causing thin and dry vaginal skin (vaginal atrophy) and the presence of a vaginal pessary, it is important to use topical vaginal estrogen creams and tablets regularly to reduce the risk of ulceration and bleeding.
This is a condition where low estrogen causes thin, dry and inflamed vaginal skin. Vaginal atrophy is common in peri-menopause or menopause women. Some doctors term this as “urogenital syndrome” due to its associated urinary symptoms, which may include burning with urination, urinary urgency, recurrent urinary tract infections (UTI) and urinary incontinence.
What are the symptoms of vaginal atrophy?
Symptoms vary widely between women and may include one or more of the following:
Vaginal dryness (both baseline and reduced lubrication during sex)
Other than menopause, are there other risk factors?
Surgical removal of both ovaries
Chemotherapy
Radiotherapy (particularly pelvic radiation treatment for cancer)
What are the complications of vaginal atrophy?
As vaginal skin is thin and dry with a rise in vaginal pH, there is an increased risk of infection including urinary tract infections, vaginal infections and bleeding after menopause. Inability to engage in sex can also cause relationship strain and affect one’s physiological well-being and self-esteem.
This is typically applied/inserted into the vagina twice weekly and restores the vaginal skin thickness and suppleness. Due to local topical application with low absorption into the body, it is safe to use long-term.
Regular sex
Sexual activity increases blood flow to your vagina and keeps atrophy at bay.
What is a urinary tract infection (UTI)?
A UTI is an infection of your urinary tract – this can involve anywhere from your kidneys, ureters (tubes connecting your kidneys and bladder), bladder, and urethra (pipe connecting your bladder to the outside). Most commonly, UTI involves the bladder.
Adult women have UTIs more often than men as their urethra is shorter and nearer to the anus, making it easier for bacteria to enter.
What are the symptoms of UTI?
Painful urination
Frequent urination (but little or no urine passed)
Blood in your urine
Pain in your lower pelvis
Fever
What are the risk factors for UTI?
Menopausal changes (vaginal atrophy): low estrogen cause tissues in the genital region to be thinner and dryer resulting in higher risk of infection
Pregnancy: suppressed immune system
Sex (in some women)
Bladder or kidney problems e.g. stones
Surgery (or having a urinary catheter placed)
Not being to empty bladder completely (retention of urine): this may be more common in women who are elderly or have medical conditions such as diabetes, dementia, stroke, previous spine surgery
What tests are needed to diagnose UTI?
You will be asked to produce a urine sample – clean your vaginal lips before passing urine and catch the middle portion of your urine stream. A microscopic analysis is first done to check for the presence of white blood cells in your urine sample, which indicates the possibility of a UTI. A urine culture is then performed over a few days to determine the bacteria in your urine (if any) and the appropriate antibiotics that kill the bacteria.
If you have recurrent UTIs (≥2 UTIs in the last 6 months or ≥3 UTIs in the last 12 months which are culture confirmed), you will need to undergo further tests which may include:
Ultrasound or CT of your kidneys and bladders
Cystoscopy (scope to check the inside of your bladder)
What is the treatment for UTI?
Your doctor will prescribe a course of oral antibiotics, which you will need to complete. Sachets that alkalinize your urine e.g. citravescent can help. Drink lots of water to dilute your urine. Occasionally, if there are no suitable oral antibiotic options for your UTI, or if your UTI is severe/complicated, you may need to be hospitalised for intravenous antibiotics.
If the issue is chronic retention of urine, urine catheters (tube to drain urine) may necessary in the short or long-term. Menopausal changes (vaginal atrophy) can be treated with topical vaginal estrogen (creams and tablets).
How do I prevent myself from getting UTIs?
Drink 7-8 cups of water every day
Drink at regular intervals (1 cup every 2-3 hourly)
Pass urine at regular intervals (every 2-3 hourly) – do not hold your bladder excessively
Avoid constipation
After using the toilet, always wipe from front to back
Avoid douching or feminine wash as it may irritate your vulva skin and increase the risk of infections
Wear cotton underwear and loose fitting clothes
Keep your diabetes under control
Lubricate during sex
Go to the bathroom before and as soon as possible after sex
Take a balanced diet and include probiotics (e.g. yakult, vitagen, yoghurt, cranberry juice etc)
What is topical vaginal estrogen?
This is a low dose, local estrogen therapy that comes in the form of creams and tablets. These are applied and inserted into the vagina respectively. It helps to relive the symptoms of vaginal atrophy by restoring the vaginal skin thickness, suppleness, addressing dryness and reducing the vaginal pH. The most common forms are Premarin cream and Vagifem tablets.
Is topical estrogen therapy safe?
As it is a local treatment i.e. applied only at the vagina, little or no estrogen is absorbed into the body. It is safe for long-term usage. Initiation therapy is usually daily for 2 weeks, followed by twice weekly dosing before bedtime for maintenance. Studies have not shown an increased risk of cancer recurrence even in women with a history of breast cancer.
How do I apply topical estrogen therapy?
Premarin cream
You may either use the applicator included in the box or your finger
Wash and dry your hands thoroughly
Apply a blueberry size (half your index finger tip) on your vaginal lips and the lower third of your vagina
Vagifem tablet
Pass urine to empty your bladder before bedtime
Wash and dry your hands thoroughly
Lie down with your knees bent and legs slightly apart
Remove pessary from wrapper
Insert pessary (pointy end first) into the vagina as far as you can manage comfortably (usually about the length of your index finger)
Wash your hands again and lie down to sleep
Notes:
Avoid sex on the nights of application/insertion .
You should try not to pass urine for at least 2-3 hours after pessary insertion. The pessary will start to dissolve once it is inserted into your vagina. It is okay if you need to get up in the middle of the night to go to the bathroom and bits of it fall out.
What is pelvic organ prolapse?
This refers to a drooping of the uterus, bladder or rectum beyond the vagina. It is more common in older women, affecting 1 in 3 women who have had children. 1 in 10 women will need surgery in their lifetime for POP.
What types of surgery are there for pelvic organ prolapse?
The type of surgery advised by your urogynaecologist will depend on your severity of pelvic organ prolapse, age, general health, medical conditions, surgical history and sexual activity. There is no one-size-fits-all. Each surgery for POP needs to be individualised. Surgery needs to done under general anaesthesia.
Vaginal pelvic reconstructive surgery
This is the most common approach as the pelvic organs are drooping out from the vagina. If the uterus is prolapsed, there is no plans for more children and the woman has no desire to keep her uterus, a vaginal hysterectomy will be performed. The ovaries can be conserved if they are normal.
Surgery for prolapse in the other compartments (pelvic floor repair) involves making a cut in the vagina and separating the prolapsed organ away from the vaginal wall. Stitches or mesh are used to strengthen the defect in the supporting tissue, and the vaginal skin is closed to reduce the bulge.
If this is done for the bladder, it is known as an anterior repair or colporraphy. If this is done for the rectum, it is known as a posterior repair or colporraphy. In some cases, additional permanent sutures may be placed to hitch the top of the vagina to a strong ligament in the pelvis to provide additional support (sacrospinous ligament fixation/SSLF). Overall, there are no cuts on the abdomen.
Risks of surgery include:
Common (affecting 1-5% of patients):
Vaginal bleeding / haematoma – in cases of significant bleeding, blood transfusion and/or additional procedures may be required to stop the bleeding
Postoperative pain (in cases of SSLF, this is usually involves the right buttock and usually resolves in a few weeks)
Urinary retention, infection, frequency, urgency, urge and urinary incontinence
Wound infection
Constipation
Difficulty and/or pain with intercourse
Failure to achieve the desired result; recurrence of prolapse
Earlier onset of menopause
Uncommon (affecting 0.1-1% of patients):
Injury to the bladder
Pelvic abscess
Venous thrombosis (Blood clot in legs) / Pulmonary embolism (Blood clot in lungs)
Rare (affecting <0.1% of patients):
Serious adverse reactions to general anaesthesia
Excessive bleeding requiring transfusion or return to theatre
Injury to the urinary tract / bowel
Admission to the intensive care unit for monitoring should the operation be of prolonged duration or result in complications
Death: the risk is approximately less than 1 in 4000
Mesh usage is typically reserved for the most severe/ recurrent cases due to permanent implantation of synthetic material. This gives a better support for POP compared to stitches, but can only be used by trained urogynaecologists in a select few. There is a risk of mesh complications such as erosion, infection, scarring and chronic pain, which may require further procedures.
Abdominal approach (sacrocolpopexy)
This is an option for women with previous hysterectomy and an apical prolapse (top of vagina collapsing downwards out of the vaginal opening). It involves making cuts in the abdomen and using a permanent synthetic mesh to hitch the vagina up to the sacrum, which is a large triangular bone at the base of the spine.
Vaginal closure surgery
In a few instances, vaginal closure surgery may be recommended for women with severe prolapse who are medically unfit for vaginal pelvic reconstructive surgery and are not sexually active. This surgery involves pushing the prolapsed organs back into the vagina and stitching the vaginal walls together.
How successful is surgical treatment for pelvic organ prolapse?
70% of women will have a long-term cure after undergoing surgery for POP. For those with permanent implantation of synthetic mesh, the success rate goes up to 90%. It is important to note that the limitation of pelvic reconstructive surgery lies in working with ageing/weakened tissues. Hence, pelvic organ prolapse typically recurs due to persistent risk factors that caused the initial prolapse. Although ageing cannot be reversed, lifestyle modifications like maintaining a healthy body mass index (BMI), avoiding chronic cough, constipation and lifting heavy loads remain essential.
It is normal to go to the toilet at night once or twice, especially as you get older. If you find yourself waking up more than 2 times at night to pass urine, you may have nocturia.
There are many causes of nocturia, which include:
High fluid intake, especially in the 2nd half of the day and before bedtime
Heart failure: where there is fluid accumulation in the body
Certain blood pressure or heart medications that prevent fluid accumulation in the body
Poor sleep quality, where one goes to the toilet frequently at night since they are already awake
Nocturia is a common and long-term condition, especially in women of older age.
What tests do I need to diagnose this?
You should consult a urogynaecologist, who is a gynaecologist specialising in female urinary disorders. Your doctor will take a detailed medical history and perform a pelvic examination to check for any pelvic organ prolapse and pelvic floor muscle tone.
Depending on your symptoms, you may require an ultrasound to check your uterus and ovaries, urine tests, bladder scan (to check the amount of urine remaining in your bladder after you have passed urine), and/or urodynamic study (this is a test to check for your bladder function and bladder muscle stability).
What is the treatment for nocturia?
You may not be fully cured because this is a long-term condition, but there are many good ways to keep your symptoms under control so that your life does not revolve around your bladder.
Conservative treatment
The first line treatment is lifestyle changes, which are sometimes sufficient to improve your symptoms significantly. You will need to fill a bladder diary to keep track of your symptoms. These include:
Adjusting your diet or fluid intake: spread your fluid intake evenly throughout the day and stop drinking 3 hours before bedtime
Cutting down on caffeinated drinks (you should not take them at all beyond late afternoon)
Pass urine just before bedtime
Avoid sleeping in air-conditioned room
Avoid drinking when you wake up at night to pass urine
Improving control of medical conditions e.g. diabetes, or changing medications after discussion with your doctor
Seek help if you have a sleep problem
For older women, it may help to sleep in a room with an attached toilet, or a commode if mobility is poor. Make sure that the route to the toilet can be well-lit and clear of obstacles to reduce the risk of falls.
Medications
If conservative treatments do not work, medications are usually prescribed in addition to the lifestyle changes above. These relax your bladder muscle and allow you to increase the intervals that you need to pass urine. The medications take some time to work so you will have to take them for at least a few months to see the full results. Side effects include giddiness (so you should take them just before going to bed), dry eyes, dry mouth, dry skin and constipation. You may have to try different drugs before finding one that suits you. There are certain medical conditions that may make you unsuitable to take these medications – do check with your urogynaecologist.
Kegel exercises are important in strengthening and maintaining your pelvic floor muscle tone. It is helpful in improving:
Kegel exercises should be started as early as possible – preferably when you get pregnant – and continued well into your menopausal years.
Here are some tips on how to do Kegel exercises:
Try and imagine that you are trying to stop a fart from coming out, or trying to stop your urine flow in the middle of the stream. You may find it useful to find the correct muscles by actually doing this while you are sitting on the toilet bowl, but do not do it routinely as you may teach your bladder bad habits!
Lie down on your bed with your knees bent and legs slightly apart
Put a small mirror in between your legs and observe your vagina and anus openings while you try and squeeze your pelvic floor muscles. You should see the openings getting smaller and being lifted in and upwards
It is normal for you to take some time to learn which are the correct muscles and how to squeeze and relax sufficiently at first. Don’t worry and be patient!
Once you have identified the correct muscles:
Squeeze your pelvic floor muscles and hold for 1 second – repeat 5 times
Squeeze and hold for 5 seconds – repeat 5 times
Step 1 + Step 2 = 1 cycle (30 seconds)
Do 5 cycles (2-3 minutes) three or four times a day (7-10 minutes)
The key is remembering to do your Kegel exercises daily. You can do them any time, in any place and in any position as nobody can tell that you are doing them! Don’t limit yourself to the sets above – if you can do it more often, do so.
If you have difficulty grasping the technique of Kegel’s exercises, speak with your gynaecologist who can refer you to a specialised physiotherapist.
As it is likely that your pelvic floor muscles have weakened, you may not see results until you have put in consistent efforts for at least 3 to 6 months. Remember – slow and steady wins the race!
Dr. Ng Kai Lyn
MBBS (SG) | MMed (SG) | MRCOG (UK) | FAMS (SG)
Empowering Women's Health
This article has been medically reviewed by Dr Ng Kai Lyn
Dr Ng Kai Lyn 黄楷伶 is a Consultant Obstetrician and Gynaecologist with sub-specialty expertise in urogynaecology and minimally invasive surgery, as well as a clinical interest in fertility.
The contents on this website provides general information only and does not replace professional or specialist advice. If you think you may have any medical condition, always seek prompt medical attention from a professional healthcare provider. It is not advisable to delay consulting professional advice by relying on the information provided here. Although reasonable efforts have been made to ensure that the information is relevant and comprehensive, we make no guarantees or representation that the contents on this website are complete, up-to-date or accurate. drngkailyn.com is independently owned and is not affiliated or endorsed by any organisation.














{kind=link}