Understanding the Impact of Adenomyosis on Periods and Reproductive Outcomes
Adenomyosis, a gynaecological condition characterised by the growth of endometrial tissue deep into the uterine muscle, has long been associated with painful periods and heavy menstrual bleeding. However, its impact on fertility is a concern for many women of reproductive age. This condition, often overshadowed by its close relative endometriosis, can significantly influence fertility, yet it remains under-discussed.
What is adenomyosis?
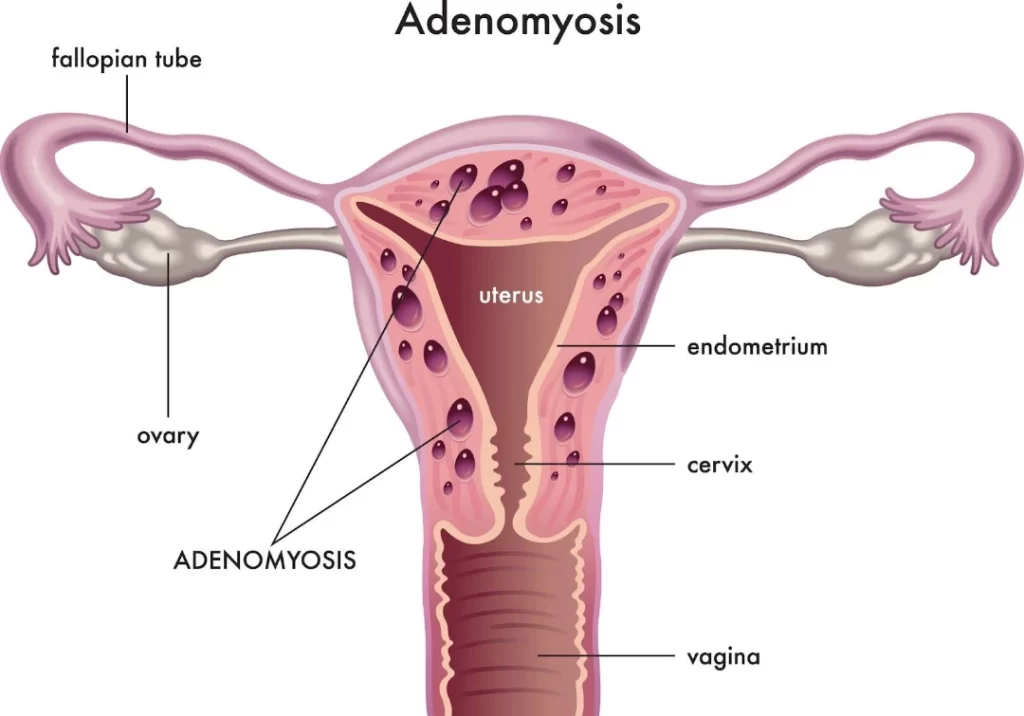
Adenomyosis, classified as a benign gynaecological disorder, is characterised by the infiltration of endometrial glands and stroma into the myometrium, the muscular layer of the uterus. This infiltration disrupts the normal architecture of the uterine wall, which results in a range of clinical symptoms, including dysmenorrhoea, heavy menstrual bleeding, pelvic pain, and, in some cases, infertility. While the exact aetiology of adenomyosis has not been fully delineated, some postulated causes and risk factors can lead to an increased chance of developing adenomyosis.
Adenomyosis is a condition where the tissue that lines the uterus grows into its muscular walls, causing pain, heavy bleeding, and potential fertility challenges.
How common is adenomyosis among women?
Adenomyosis is relatively common, affecting between 8% and 31% of women [1], though exact prevalence rates can vary. It most commonly occurs in women aged 40 to 50 but can also affect younger women. The condition is often underdiagnosed because its symptoms can overlap with other gynaecological issues, such as endometriosis and fibroids.
What is the root cause of adenomyosis?
The exact cause of adenomyosis remains unclear, but several theories and factors have been proposed to explain its development:
Invasive tissue growth: one of the leading theories is that adenomyosis results from the direct invasion of endometrial cells into the myometrium, the muscle layer of the uterus. Anything that injures the myometrium can further promote this, such as uterine incisions during caesarean sections, myomectomies [2], and dilation and curettage (D&Cs) [3].
Developmental origins: another theory suggests that adenomyosis may originate during foetal/embryonic development, where the endometrial tissue becomes embedded within the uterine muscle.
Hormonal factors: the role of oestrogen seems significant, as adenomyosis is common in women during their reproductive years when oestrogen levels [4] are higher; oestrogen is known to stimulate the growth of endometrial tissue.
Inflammation:chronic inflammation [5] in the uterus may also play a role in the development of adenomyosis. Another theory suggests a link between postpartum inflammation of the uterine lining, which results in a break in the boundary between the endometrium and myometrium and causes adenomyosis to develop.
Immune system dysfunction: some researchers [6] believe an impaired immune response might fail to eliminate ectopic endometrial cells that grow within the myometrium, allowing adenomyosis to develop.
Understanding of adenomyosis is constantly evolving. It is still poorly understood, and multiple factors likely contribute to its development; as such, much research is still ongoing.
What are the symptoms of adenomyosis?
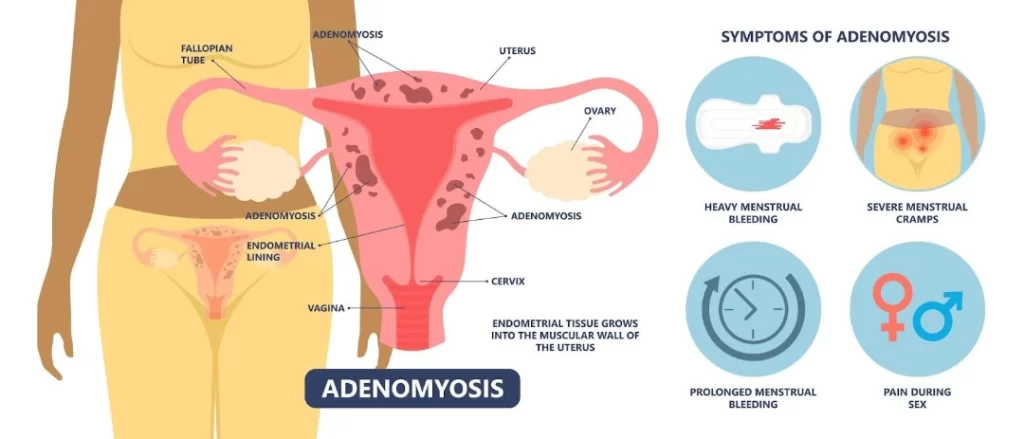
The symptoms of adenomyosis can vary widely among individuals and may also overlap with other gynaecological conditions. However, common symptoms associated with adenomyosis include:
Menstrual irregularities: this commonly includes heavy menstrual bleeding (menorrhagia) [7], which can manifest in heavy flow requiring frequent pad changes and clot passage and sometimes can result in iron deficiency anaemia if this is long-standing.
Pelvic pain/dysmenorrhea: women with adenomyosis often experience pelvic pain that can range from dull and constant to sharp and severe. The pain is usually more pronounced at the lower abdomen/pelvic region just before or during menstruation (dysmenorrhoea) [8] or sometimes around the lower back as well; some women may require analgesia to help manage the menstrual cramps.
Abdominal discomfort: some individuals may experience generalised abdominal discomfort or bloating, particularly during menstruation if the uterus has become bulky as a result of the adenomyosis.
Enlarged uterus: adenomyosis can cause the uterus to become enlarged beyond its usual size. This enlargement can sometimes be palpable either during an abdominal or, more accurately, through a bimanual pelvic exam [9]. A significantly enlarged uterus, other than resulting in menstrual disturbances highlighted above, can sometimes result in pressure symptoms on adjacent organs such as the bladder and bowels and cause issues such as urinary frequency/urgency or constipation. In extreme circumstances where the uterus is significantly enlarged, it can sometimes increase one’s risk of developing deep vein thrombosis (DVT).
Painful intercourse:dyspareunia, or pain during sexual intercourse, can sometimes occur due to the inflammation and uterine bulkiness associated with adenomyosis; however, this more commonly manifests in patients with endometriosis.
Heavy menstrual bleeding is a common symptom of adenomyosis, often resulting in significantly heavier flow and/or painful periods.
It’s important to note that not all individuals with adenomyosis will experience severe symptoms. Some women may have mild symptoms or be completely asymptomatic. Yet others may mistakenly accept their longstanding heavy menstrual flow as usual and only get flagged up when their routine health screening flags them up as being anaemic. Additionally, these symptoms can mimic other conditions, such as endometriosis or fibroids, making accurate diagnosis challenging without proper evaluation by an experienced gynaecologist.
How do I know if I have adenomyosis?
Confirming adenomyosis typically involves a combination of clinical evaluation, imaging studies, and, sometimes, histological examination. Here are the common methods used to confirm adenomyosis:
Clinical evaluation: your healthcare provider will begin by taking a detailed medical history and conducting a physical examination. During the pelvic exam, they may palpate an enlarged and tender uterus, which can be indicative of adenomyosis.
Imaging studies:
Transvaginal ultrasound (TVUS): this is often the initial and most common imaging modality used to evaluate adenomyosis. A transvaginal ultrasound provides better resolution than a transabdominal ultrasound and may reveal a larger-than-normal uterus, with diffuse thickening of the myometrium that can sometimes be asymmetrical; in some cases where the adenomyosis is more focal, more distinct adenomyomas with ill-defined margins may be appreciable.
Magnetic resonance imaging (MRI): MRI is another valuable tool for diagnosing adenomyosis, especially when TVUS results are inconclusive or further clarification is needed. MRI typically looks for similar features outlined in the ultrasound scan, with further delineation on junctional zone thickening (the transition area between endometrial and myometrial layer).
Histological examination: in some cases, a definitive diagnosis of adenomyosis may only be revealed on histological examination of uterine tissue obtained through procedures such as myomectomy/hysterectomy, as early adenomyosis may be microscopic.
It’s important to note that adenomyosis can sometimes coexist with other uterine conditions, such as fibroids or endometriosis, which further emphasises the need for a thorough evaluation by a gynaecologist experienced in diagnosing and managing these conditions.
Adenomyosis frequently presents with period problems.
How does adenomyosis impact fertility outcomes?
Adenomyosis can significantly impact fertility outcomes through various mechanisms that affect the reproductive process. Here are some ways in which adenomyosis influences fertility:
Impaired endometrial receptivity: adenomyosis can disrupt the normal architecture and function of the endometrium, the inner lining of the uterus where embryo implantation occurs. The presence of adenomyotic lesions within the endometrium may interfere with the normal hormonal and molecular signalling pathways involved in embryo attachment and implantation.
Distorted uterine cavity: adenomyosis (which may be asymmetrical) and thickening of the uterine walls can distort the uterine cavity [10]. This distortion may interfere with embryo implantation and development or increase the risk of miscarriage.
Increased risk of miscarriage: women with adenomyosis may have a higher risk of miscarriage [11] compared to those without the condition – the exact reasons for this association are not fully understood but may be related to abnormalities in the endometrium or uterine function.
Co-existence with endometriosis/uterine fibroids with reduced fertility rates:studies [12] have shown that adenomyosis is associated with reduced fertility rates, including decreased chances of spontaneous conception and higher rates of infertility. The presence of multiple concurrent conditions, such as endometriosis and uterine fibroids, may also compound the effects on fertility and make conception more challenging.
It is important to note, however, that not all women with adenomyosis will experience fertility issues – many with adenomyosis go on to conceive without difficulty. However, for those who have fertility issues and/or have been diagnosed with adenomyosis, it is important to work closely with a gynaecologist to develop an individualised treatment plan to address both problems.
How does adenomyosis affect pregnancy?
Adenomyosis can have various effects on pregnancy, presenting unique challenges and potential complications for individuals with this condition. Women with adenomyosis are at increased risk of various adverse obstetric outcomes [13], including:
Miscarriage: women with adenomyosis are at an increased risk of miscarriage.
Pre-eclampsia: this is a condition during pregnancy where the expectant mother develops high blood pressure associated with proteinuria
Preterm birth: the risk of preterm birth [14], when the baby is born before completing 37 weeks gestational age, is increased in women with adenomyosis.
Low birth weight/small for gestational age: this is when the baby’s weight is lower than expected.
Postpartum haemorrhage: women with adenomyosis may experienceexcessive bleeding following childbirth/delivery.
It is important for individuals with adenomyosis who are planning a pregnancy or are already pregnant to work closely with their obstetrician to address any potential risks, monitor for complications, and optimise care to promote a healthy pregnancy and delivery.
What is the best treatment for adenomyosis?
The best treatment for adenomyosis depends on factors such as the severity of the symptoms, the patient’s age, whether fertility preservation is desired, and the individual’s overall health. Treatment options vary from conservative management to surgical interventions.
Pain management
Nonsteroidal Anti-Inflammatory Drugs (NSAIDs): these are commonly prescribed to reduce menstrual pain and inflammation. They are most effective when taken before the onset of symptoms.
Tranexamic acid tablets: these are taken on heavy menstrual flow days (on an as-needed basis) to help alleviate excessive menstrual blood loss
Hormonal treatments:
Oral contraceptives: birth control pills can help regulate the menstrual cycle and reduce the heavy bleeding and pain associated with adenomyosis.
Progestin therapy: this includes options such as intrauterine devices (IUDs) that release progestin, such as Mirena, which helps to reduce menstrual cramps and heavy bleeding.
Gonadotropin-Releasing Hormone (GnRH) Agonists: these drugs can induce a temporary menopause-like state, reducing estrogen production and often leading to symptom relief; however, these are typically reserved only for a small subset of suitable patients.
Uterine-sparing surgical options
Uterine artery embolisation: this involves cannulating either the femoral or radial artery to reach the uterine arteries (blood vessels that supply the uterus) to release embolic substances to occlude the blood supply to the uterus, hence achieving an overall shrinkage of the adenomyotic uterus. An interventional radiologist typically performs this as a day surgery procedure and may be associated with certain risks, including premature menopause, and is hence not usually recommended for women still desiring fertility; there is also a risk of symptomatic recurrence requiring additional treatments downstream.
HIFU (high-intensity focus ultrasound): HIFU involves using thermal ablation to induce coagulative necrosis of the adenomyotic uterus. It is not widely available in Singapore and does not allow for complete clearance of all adenomyosis. Hence, it has a risk of symptomatic recurrence, requiring additional treatments downstream.
Adenomyomectomy: this surgery involves removing the bulk of adenomyotic tissue from the uterus. It can be effective but requires careful execution to preserve uterine integrity (hence may not be the first line for women still desiring fertility) and is associated with a significant risk of recurrence due to the difficulty of complete resection given the microscopic nature of endometrial tissue invasion into the myometrium that can not be discerned with the naked eye intra-operatively.
Total hysterectomy
Total hysterectomy, which involves the removal of the uterus, is the only definitive cure for adenomyosis. This option is typically considered for women who have severe symptoms, have completed childbearing, or when other treatments have failed; surgical approaches of either laparotomy (open) or laparoscopy (key-hole/minimally invasive) options depend on the size of the enlarged uterus.
Lifestyle changes
These can help manage/alleviate the symptoms of adenomyosis but do not serve to cure adenomyosis.
Diet and nutrition: eating a balanced diet rich in anti-inflammatory foods can help manage symptoms. Some women find relief by reducing their intake of processed foods and increasing their intake of foods rich in omega-3 fatty acids.
Physical therapy: pelvic floor physical therapy can help manage pain and improve pelvic muscle function.
Acupuncture and herbal remedies: some women find these traditional treatments, e.g. TCM helpful for managing their symptoms.
Conclusion
In conclusion, adenomyosis, though often overshadowed by its counterpart endometriosis, significantly impacts fertility and reproductive health. This condition, characterised by the infiltration of endometrial tissue into the uterine muscle, presents a range of symptoms, including painful periods, heavy bleeding, and pelvic discomfort. Despite its prevalence among women, adenomyosis remains underdiagnosed and under-discussed.
In essence, raising awareness about adenomyosis, promoting early detection, and implementing comprehensive management strategies are essential steps toward addressing its impact on women’s quality of life, fertility and reproductive outcomes for affected individuals. By fostering a deeper understanding of this condition within medical communities and among women, we can empower individuals to navigate their women’s health journey with confidence and informed decision-making.
Orazov, M. R., Radzinsky, V. E., Nosenko, E. N., Khamoshina, M. B., Dukhin, A. O., & Lebedeva, M. G. (2017). Immune-inflammatory predictors of the pelvic pain syndrome associated with adenomyosis . Gynecological Endocrinology, 33(sup1), 44–46. https://doi.org/10.1080/09513590.2017.1399696
d’Otreppe J, Patino-García D, Piekos P, de Codt M, Manavella DD, Courtoy GE, Orellana R. Exploring the Endocrine Mechanisms in Adenomyosis: From Pathogenesis to Therapies. Endocrines. 2024; 5(1):46-71. https://doi.org/10.3390/endocrines5010004
Huang, Y., Zhao, X., Chen, Y., Wang, J., Zheng, W., & Cao, L. (2020). Miscarriage on Endometriosis and Adenomyosis in Women by Assisted Reproductive Technology or with Spontaneous Conception: A Systematic Review and Meta-Analysis. BioMed research international, 2020, 4381346. https://doi.org/10.1155/2020/4381346
Harada, T., Khine, Y. M., Kaponis, A., Nikellis, T., Decavalas, G., & Taniguchi, F. (2016). The Impact of Adenomyosis on Women’s Fertility. Obstetrical & gynecological survey, 71(9), 557–568. https://doi.org/10.1097/OGX.0000000000000346
Vercellini, P., Viganò, P., Bandini, V., Buggio, L., Berlanda, N., & Somigliana, E. (2023). Association of endometriosis and adenomyosis with pregnancy and infertility. Fertility and sterility, 119(5), 727–740. https://doi.org/10.1016/j.fertnstert.2023.03.018
This article has been medically reviewed by Dr Ng Kai Lyn
Dr Ng Kai Lyn 黄楷伶 is a Consultant Obstetrician and Gynaecologist with sub-specialty expertise in urogynaecology and minimally invasive surgery, as well as a clinical interest in fertility.
The contents on this website provides general information only and does not replace professional or specialist advice. If you think you may have any medical condition, always seek prompt medical attention from a professional healthcare provider. It is not advisable to delay consulting professional advice by relying on the information provided here. Although reasonable efforts have been made to ensure that the information is relevant and comprehensive, we make no guarantees or representation that the contents on this website are complete, up-to-date or accurate. drngkailyn.com is independently owned and is not affiliated or endorsed by any organisation.