Uterine fibroids are benign (noncancerous) tumours that develop in the uterus and are a common condition affecting a significant proportion of women during their child-bearing, i.e. reproductive years. These growths arise from the muscle layer of the uterus and can vary in size, from as small as a pea to as large as a melon. They may grow singularly or in multiple numbers and can affect different locations of the uterus – the location of fibroids can influence the symptoms a woman experiences as well as the treatment options. Fibroids are known to exhibit slow growth over the years and will usually start shrinking following menopause.
Uterine fibroids are noncancerous uterine growths commonly occurring during a woman’s reproductive years.
How common are uterine fibroids, and who is at the most risk?
Uterine fibroids are quite common, affecting most women by the age of 50 [1]. The prevalence can vary based on age, ethnic background, genetic factors, and lifestyle. They are most commonly diagnosed in women in their 30s and 40s. Factors that increase the risk of developing uterine fibroids include:
Ethnicity:African-American women are more likely to develop fibroids compared to women of other racial and ethnic backgrounds [2].
Family history: there is a higher risk for women who have a family member with fibroids to develop uterine fibroids themselves, as there seems to be a genetic predisposition to this [3].
Lifestyle and environmental factors: although the exact mechanisms of lifestyle and environmental factors that contribute to the risk of developing uterine fibroids are poorly understood, poor diet (e.g., high in red meats and low in fruits/vegetables/fibre) [5], lack of exercise (e.g., sedentary lifestyle) [6], stress [7], alcohol consumption [8], etc., may contribute to the risk of developing fibroids.
Age: fibroids are commonly diagnosed in women between the ages of 30 and 50, although they can develop/occur at any age [9].
Hormonal factors: fibroids tend to grow over the years, with expedited growth during pregnancy [10] (when hormonal levels are high), and occasionally also demonstrate increased growth when one is on hormone replacement therapy (HRT) [11]. Fibroids then commonly shrink over time after a woman attains menopause as hormonal levels decline.
The exact cause of uterine fibroids is still unknown, and the majority of women who have them do not have any of the above risk factors. Regular gynaecological check-ups can help in the early detection and management of uterine fibroids. It is also important to monitor one’s menstrual cycles closely and seek medical attention early should changes be detected.
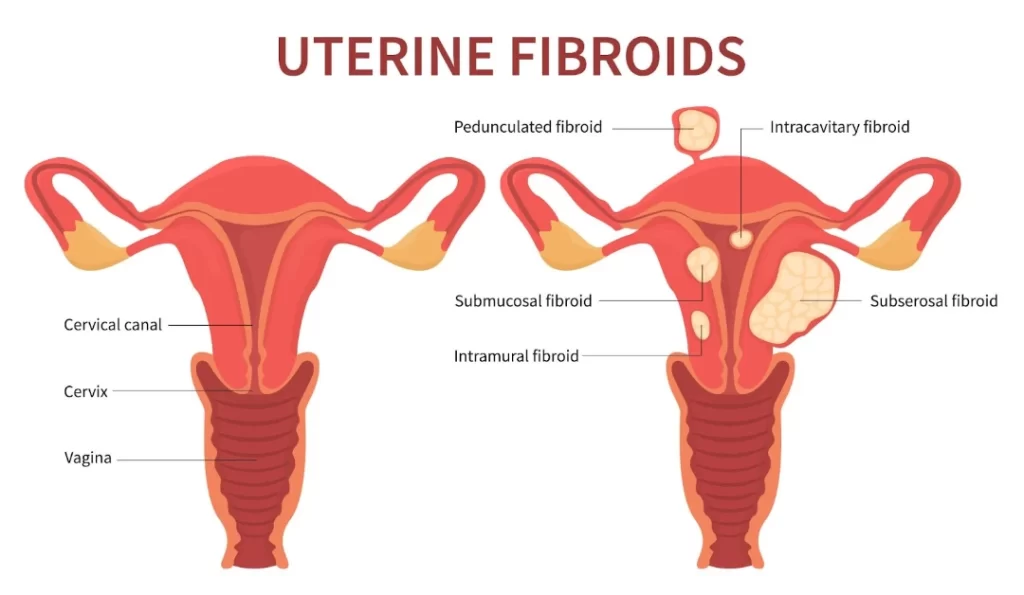
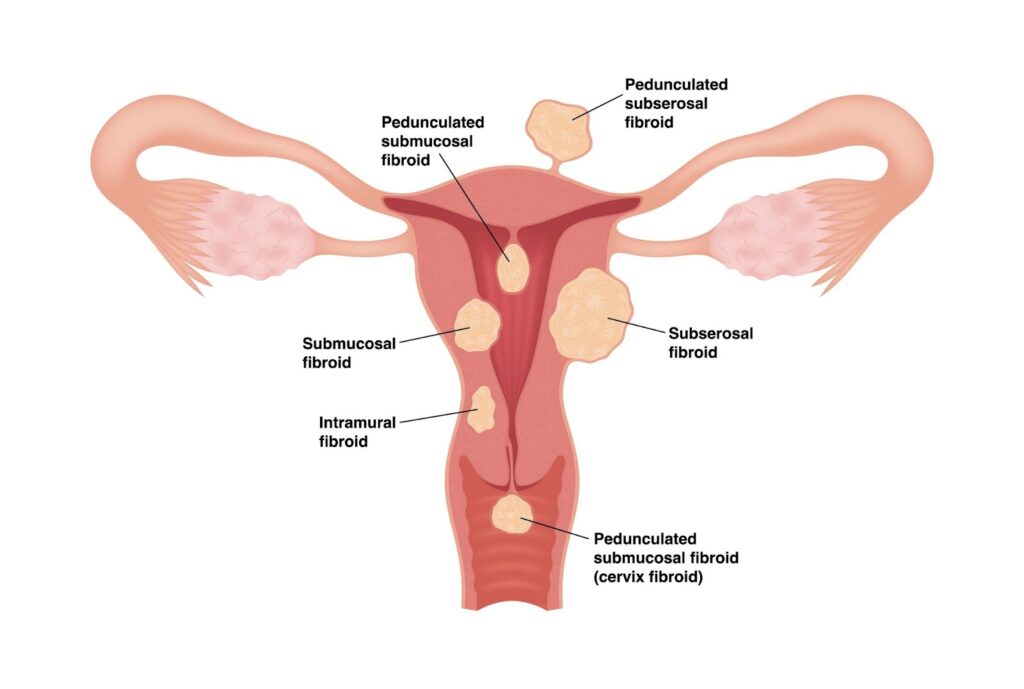
What types of uterine fibroids exist?
Uterine fibroids are generally categorised based on their location within the uterus, leading to different types:
Intramural fibroids are the most common type of fibroids, developing within the muscular wall of the uterus [12]. They can grow larger and cause a larger uterine size than usual, resulting in heavy menstrual bleeding.
Subserosal fibroids: these fibroids grow/develop on the outer serosal layer of the uterus and, depending on their size, can result in extrinsic pressure on surrounding/adjacent organs such as the bladder (leading to urinary frequency, urgency or sensation of incomplete emptying) or the rectum (leading to constipation), or simply pelvic heaviness or a palpable pelvic-abdominal mass [13]. They may be connected to the uterus by a narrow stalk, which is why they are called pedunculated fibroids.
Submucosal fibroids: less common than the other types, these fibroids develop in the submucosal layer (the innermost layer) of the uterus [14]. They can protrude into the uterine cavity, leading to heavy/prolonged/frequent/unscheduled menstrual bleeding as well as fertility issues.
Pedunculated fibroids:pedunculated fibroids grow on a stalk either inside the uterine cavity (pedunculated submucosal) or on the outer surface of the uterus (pedunculated subserosal) [15]. They can sometimes twist, causing severe pain and necessitating emergency treatment.
Cervical fibroids:cervical fibroids occur in the cervix, the lower part of the uterus, and are relatively rare compared to the other types [16].
Uterine fibroids are categorised into different types based on their location.
The location and size of the fibroids significantly influence the symptoms they may cause and the treatment options available. Some fibroids involve more than one location, i.e. transmural and may be challenging to treat.
Are uterine fibroids benign or malignant?
Uterine fibroids are benign, which means they are noncancerous growths. They originate from the muscle tissue of the uterus, and while they can vary in size and number, they do not spread to other parts of the body as malignant (cancerous) tumours would.
Although fibroids are not associated with an increased risk of uterine cancer and are almost always benign (over 99% of fibroids are benign), they can still cause significant health issues, including menstrual disturbances such as heavy menstrual bleeding, pelvic pain, and pressure symptoms affecting the bladder or rectum. However, a small proportion of fibroids may rarely undergo malignant transformation to become cancerous – these usually present with rapidly enlarging size of fibroids and are termed leiomyosarcoma [17].
How can uterine fibroids be distinguished from uterine cancer?
Uterine fibroids and uterine cancer, such as endometrial cancer or leiomyosarcoma, can have different symptoms and characteristics. Fibroids often cause symptoms like abnormal uterine bleeding. At the same time, uterine cancer may present with similar symptoms. Still, it may also include rapidly enlarging the size of fibroids and other constitutional symptoms such as loss of appetite, weight loss, etc.
To differentiate between fibroids and cancer, the following diagnostic methods are commonly used:
Ultrasound: a pelvic ultrasound is often the first step in evaluating the presence of fibroids and can help distinguish them from other types of growths.
Magnetic resonance imaging (MRI): an MRI can provide detailed images of the uterus, helping to identify the nature of the growths and distinguish between benign fibroids and potential malignancies.
Endometrial biopsy: an endometrial biopsy involves obtaining a sample of the endometrium (the lining of the uterus) and examining it for abnormal cells. This can help diagnose uterine cancer.
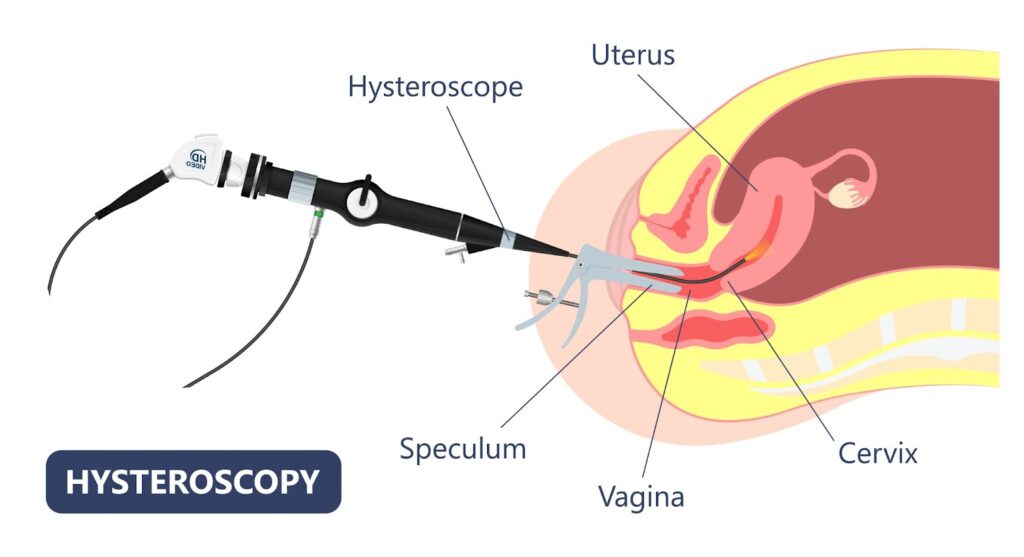
Hysteroscopy: a hysteroscopy is a procedure where a small camera is inserted into the uterus to directly visualise the uterine cavity, which can help identify abnormal growths and allow for biopsy.
It is through a combination of these diagnostic methods, along with a thorough medical history and examination, that doctors can differentiate between uterine fibroids and cancer.
A hysteroscopy involves inserting a small camera into the uterus to visualise the uterine canal.
How are uterine fibroids managed and treated?
Uterine fibroids can be managed and treated using various approaches, depending on the size and location of the fibroids, the severity of symptoms, the woman’s age, and her desire for future pregnancies. Treatment options range from watchful waiting to medication and surgery:
Watchful waiting: many fibroids are asymptomatic and do not require immediate treatment. In these cases, regular monitoring of the fibroid’s size and symptoms may be all that is needed.
Medications
Nonsteroidal anti-inflammatory drugs (NSAIDs):NSAIDs can be used to relieve menstrual cramps, which may be associated with fibroids; however, they only serve as symptomatic relief and do not reduce fibroid size.
Tranexamic acid tablets: these are oral fibrinolytic tablets that can help alleviate heavy menstrual flow and clot passage; however, they only serve as symptomatic relief and do not reduce fibroid size.
Oral contraceptive pills: thesecan help alleviate both heavy menstrual bleeding and cramps and also provide other functions such as menstrual regulation and birth control; however, they do not reduce fibroid size.
Levonorgestrel intrauterine device (IUD):IUD can be effective in reducing heavy menstrual bleeding and cramps caused by fibroids [18]; however, they can only be inserted in selected cases where the uterus is not too enlarged from fibroids, and there are no submucosal fibroids present that distort the endometrial cavity. It is also able to provide contraception at the same time.
Hormonal injection: medications like gonadotropin-releasing hormone (GnRH) agonists (usually administered via intramuscular injections) can shrink fibroids by reducing oestrogen and progesterone levels, but they are typically used only short-term due to potential side effects such as hot flushes, mood swings, bone mineral density loss, etc. There is also a risk of rebound fibroid growth following cessation of GnRH therapy. They are, hence, sometimes given as an adjuvant preoperative measure in an attempt to temporarily shrink fibroids before going in for definitive surgical management.
Non-surgical procedures
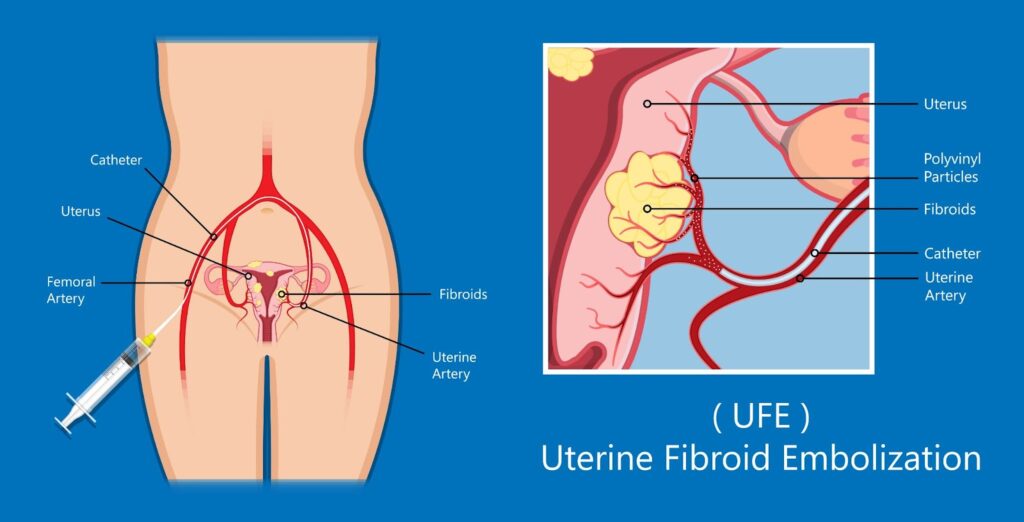
Uterine artery embolisation (UAE): a minimally invasive procedure where small particles are injected into the arteries supplying the fibroids, cutting off their blood supply and causing them to shrink. An interventional radiologist usually does this as a day surgery procedure and may require sedation. Women typically experience good short-term relief of their symptoms as their fibroids shrink (different fibroid locations may respond differently to UAE); however, due to a significant risk of fibroid regrowth with a lack of long-term efficacy, there is a significant proportion of women who will require downstream repeated treatment(s) and ultimately end up in definitive surgical management.
High-intensity focused ultrasound/MRI-guided focused ultrasound surgery (HIFU/MRgFUS): HIFU/MRgFUS uses high-frequency ultrasound sound waves to heat fibroid tissue, with the heat resulting in destruction/ablation of the targeted fibroid tissue; however, only certain fibroid locations are more amenable to this treatment modality as there is a risk of inadvertent injury to surrounding organs otherwise. Again, whilst this is a minimally invasive option and women typically experience good short-term relief of their symptoms as their fibroids shrink, due to a significant risk of fibroid regrowth with a lack of long-term efficacy, there is a significant proportion of women who will require downstream repeated treatment(s) and ultimately end up in definitive surgical management.
Uterine fibroid embolisation/uterine artery embolisation is a minimally invasive procedure that cuts off fibroids’ blood supply.
Surgical options
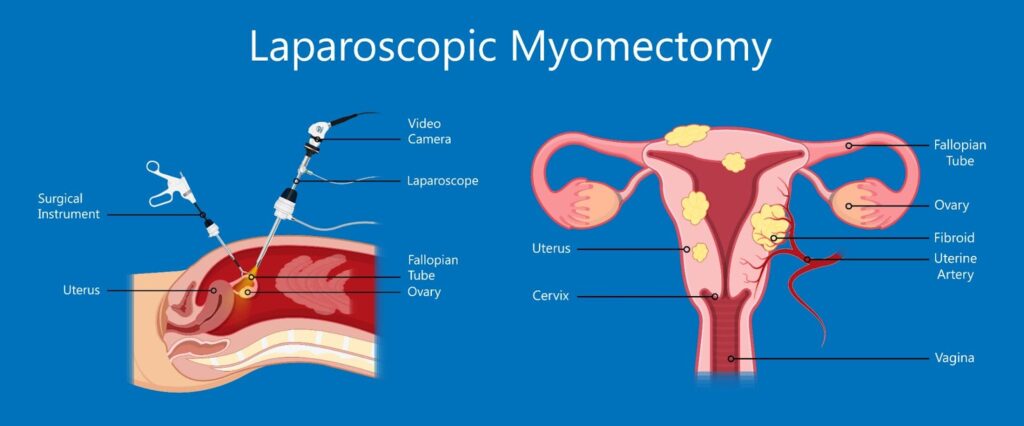
Myomectomy:myomectomy is the surgical removal of fibroids while leaving the uterus in place. This is typically the preferred surgical option for women still desiring fertility or preferring uterine conservation. Myomectomy can be done either via the open/laparotomy approach or, more commonly, through the laparoscopic approach – the best surgical approach is usually individualised. It depends on variables such as the size, number, and location of fibroids/uterus. However, myomectomy is associated with an increased risk of haemorrhage (intra-operative blood loss) as well as fibroid recurrence compared to a hysterectomy (see below); one is typically also advised to avoid conceiving within 6-12 months of a myomectomy to reduce risk of pregnancy complications. Women with previous myomectomies may sometimes be advised to consider caesarean sections as their future mode of delivery, depending on the size and location of fibroids removed.
Transcervical (hysteroscopic) resection of myoma: this treatment modality is specifically for submucous fibroids, where a hysteroscopy is introduced through the vaginal canal via the cervical canal into the uterine cavity. A resectoscope is typically used to cut the submucous fibroid into smaller chips, which are, in turn, removed from the uterus vaginally. This procedure is generally performed as a day surgery.
Hysterectomy: a hysterectomy is the complete surgical removal of the uterus. This is considered a definitive treatment for fibroids (with no future risk of fibroid recurrence) and is suitable for women who have completed their family and are no longer desiring fertility. Following a hysterectomy, one will no longer have periods nor have the ability to carry pregnancies. A hysterectomy may be done either via the open/laparotomy approach or, more commonly, through the laparoscopic approach. The best surgical approach is usually individualised and depends on different variables, such as the size and mobility of the uterus. It is commonly done in conjunction with bilateral salpingectomy (removal of both fallopian tubes, as the tubes are attached to the uterus). Depending on age and preferences, ovaries can be conserved during a hysterectomy. If the ovaries are conserved, one will continue to have normal levels of female hormones and will not be deemed menopausal (even if there are no longer periods). If the ovaries are removed at the same setting as a hysterectomy, then one will be considered to be surgically menopausal.
Laparoscopic myomectomy is a minimally invasive surgical procedure used to remove uterine fibroids through small incisions, resulting in less pain and a quicker recovery.
Lifestyle and alternative treatments
Diet and exercise:evidence suggests that maintaining a healthy weight and following a diet low in red meat and high in green vegetables may help manage symptoms [19].
Alternative medicine: acupuncture, herbal remedies, and yoga may provide symptom relief for some women, but more research is needed to confirm their efficacy.
It is important to note that whilst lifestyle and alternative treatments can help alleviate symptoms arising from uterine fibroids, they do not shrink fibroids or make them disappear. The choice of definitive treatment depends on various factors, and a gynaecologist can recommend the best option based on the individual’s condition and preferences. Regular follow-ups are important to monitor the fibroids and adjust treatment as necessary.
References
Anne Zimmermann, D. B. (2012). Prevalence, symptoms and management of uterine fibroids: an international internet-based survey of 21,746 women. BMC Women’s Health, doi: 10.1186/1472-6874-12-6.
Elizabeth A. Stewart, W. K. (2013). The Burden of Uterine Fibroids for African-American Women: Results of a National Survey. Journal of Women’s Health, doi: 10.1089/jwh.2013.4334.
Veronica Medikare, L. R. (2011). The Genetic Bases of Uterine Fibroids; A Review. Journal of Reproduction and Infertility, 181-191.
Qiwei Yang, M. C. (2022). Comprehensive Review of Uterine Fibroids: Developmental Origin, Pathogenesis, and Treatment. Endocrine Reviews, doi: 10.1210/endrev/bnab039.
Andrea Tinelli, M. V. (2021). Uterine Fibroids and Diet. International Journal of Environmental Research and Public Health, doi: 10.3390/ijerph18031066.
Yunrui Sun, X. H. (2023). Association between leisure sedentary behaviour and uterine fibroids in non-menopausal women: a population-based study. BMJ Open, doi: 10.1136/bmjopen-2023-073592.
Anissa I. VINES, M. T. (2011). The Association between Self-Reported Major Life Events and the Presence of Uterine Fibroids. Women’s Health Issues, doi: 10.1016/j.whi.2010.03.009.
Hajra Takala, Q. Y.-H. (2020). Alcohol Consumption and Risk of Uterine Fibroids. Current Molecular Medicine, doi: 10.2174/1566524019666191014170912.
Zheng Lou, Y. H. (2023). Global, regional, and national time trends in incidence, prevalence, years lived with disability for uterine fibroids, 1990–2019: an age-period-cohort analysis for the global burden of disease 2019 study. BMC Public Health.
Mihaela Camelia Tîrnovanu, L. L. (2022). Uterine Fibroids and Pregnancy: A Review of the Challenges from a Romanian Tertiary Level Institution. Healthcare (Basel), doi: 10.3390/healthcare10050855.
Elisa Moro, E. D. (2019). The Impact of Hormonal Replacement Treatment in Postmenopausal Women with Uterine Fibroids: A State-of-the-Art Review of the Literature. Medicina (Kaunas), doi: 10.3390/medicina55090549.
Wojciech Wrona, A. S. (2017). The role of levonorgestrel intrauterine systems in the treatment of symptomatic fibroids. Menopause Review, doi: 10.5114/pm.2017.72758.
This article has been medically reviewed by Dr Ng Kai Lyn
Dr Ng Kai Lyn 黄楷伶 is a Consultant Obstetrician and Gynaecologist with sub-specialty expertise in urogynaecology and minimally invasive surgery, as well as a clinical interest in fertility.
The contents on this website provides general information only and does not replace professional or specialist advice. If you think you may have any medical condition, always seek prompt medical attention from a professional healthcare provider. It is not advisable to delay consulting professional advice by relying on the information provided here. Although reasonable efforts have been made to ensure that the information is relevant and comprehensive, we make no guarantees or representation that the contents on this website are complete, up-to-date or accurate. drngkailyn.com is independently owned and is not affiliated or endorsed by any organisation.