

Have you been feeling discomfort in your lower abdomen, leaking a bit when you laugh or cough, or even struggling with a nagging sensation of pressure sensation “down below” that just won’t go away? These are symptoms which many women experience but often brush aside, thinking it’s just a normal part of ageing or life after childbirth. But what if it’s more than that?
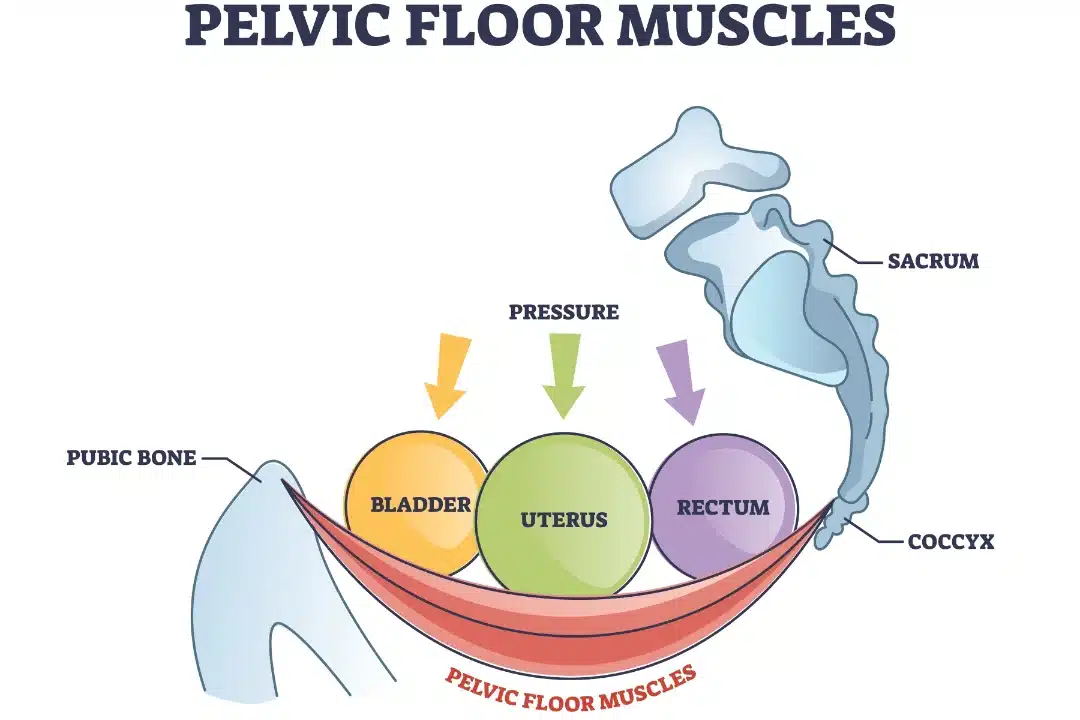
Your pelvic floor is a powerful, yet often overlooked, set of muscles that play a crucial role in supporting your pelvic organs, which consist of your bladder, uterus and rectum. When functioning properly, these muscles help you control urination, bowel movements and even sexual function. However, when the pelvic floor is weakened or damaged, it can lead to a variety of issues that fall under the category of pelvic floor disorders or pelvic floor dysfunction (PFDs).
Despite being common, many women go years without realising they’re suffering from a pelvic floor disorder as the symptoms can be subtle, slow to develop, or mistaken for other conditions. In this article, we will highlight five key signs that you might have a pelvic floor disorder—so you can stop guessing and start seeking the right help.
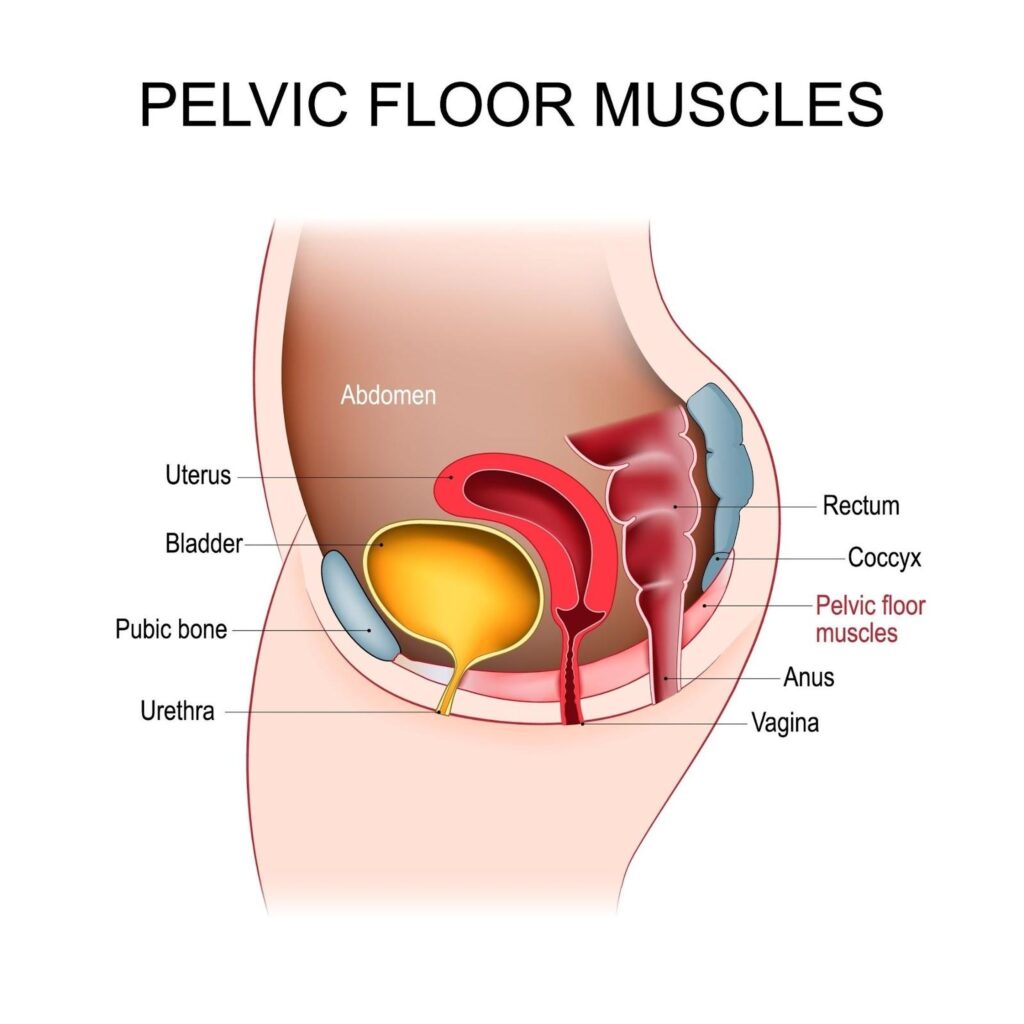
A pelvic floor disorder (PFD) occurs when the muscles and connective tissues in the pelvic area weaken, become overly tight or lose their ability to support the pelvic organs effectively. The pelvic floor is a complex network of muscles and ligaments that forms a hammock-like structure at the base of your pelvis. Its primary function is to support organs like the bladder, uterus and rectum and ensure they function properly. The pelvic floor muscles are also responsible for controlling bladder and bowel movements, as well as playing a key role in sexual function.
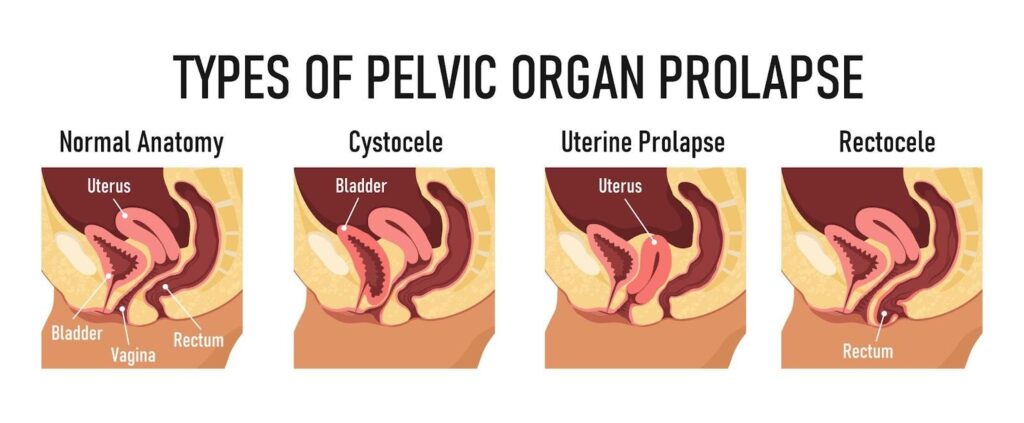
When these muscles are compromised—either through weakening, excessive strain or damage—they may not be able to perform their role efficiently leading to a pelvic floor disorder. This can result in issues like urinary incontinence, pelvic organ prolapse (when the organs drop and push against the vaginal walls) and chronic pain in the pelvic region.
Some of the most common causes of pelvic floor disorders include:
While it’s true that pelvic floor disorders are more commonly diagnosed in older women, they are not exclusive to this group. Women of all ages can experience pelvic floor issues, particularly those who have gone through childbirth, are overweight or engage in activities that put stress on the pelvic region. Young, active women can also suffer from pelvic floor disorders due to high-impact sports or improper lifting techniques.
Recognising the signs of a pelvic floor disorder (PFD) can help you seek treatment early and improve your quality of life. Here are five common symptoms that may indicate a problem with your pelvic floor:
One of the most common signs of pelvic floor dysfunction is urinary or bowel incontinence, particularly stress incontinence. This happens when the pelvic floor muscles fail to adequately support the bladder or rectum, leading to accidental leaks. You might notice this during simple activities like sneezing, coughing, laughing, jumping or exercising.
For many women, a little leakage here and there might seem harmless—perhaps you may be laughing with friends or lifting weights at the gym when it happens. However, even occasional leaks can indicate a weakened pelvic floor. While this may be brushed off as a “normal” part of ageing or post-childbirth life, it is a sign of stress incontinence and should not be ignored. Treatment options can significantly reduce/eliminate this symptom and prevent this from getting worse with time.

Another common symptom of a pelvic floor disorder is a persistent feeling of pressure or heaviness in the pelvic area. This can be a sign of pelvic organ prolapse, where one or more organs (bladder, uterus, or rectum) begin to slip out of place and push against the vaginal walls.
Women often describe this feeling as a sensation of “something falling out” or a heaviness that worsens after standing for long periods or towards the end of the day. This symptom is frequently ignored because it may come and go, but pelvic organ prolapse is a serious condition that can lead to further complications if left untreated. Early recognition can help prevent the need for surgical intervention.
If you experience pain during intercourse, known as dyspareunia, this could be another sign of pelvic floor dysfunction. Tight or overactive pelvic floor muscles can cause discomfort or pain during penetration, which makes sex unpleasant or even unbearable for some women.
The emotional toll of painful intercourse can be significant, leading to feelings of embarrassment, frustration or guilt. Over time, this may strain relationships or pose challenges in trying for pregnancy. Some women may feel ashamed to talk about it, fearing it’s an issue they have to live with. However, this is a common and treatable condition. Pelvic floor physiotherapy and other medical interventions can help alleviate the pain and restore a fulfilling sexual experience.
Another red flag for a pelvic floor disorder is difficulty in completely emptying the bladder or bowels. You may feel like you need to strain or push harder than usual to urinate or have a bowel movement, or experience a constant urge to go, even when your bladder or bowel is not full.
These issues can be frustrating and disruptive to daily life. Imagine being out at a social event, constantly feeling the need to visit the restroom, or experiencing the discomfort of never quite finishing a bowel movement. These symptoms not only affect physical health but also cause emotional stress. Treatment can address these issues and provide relief.
Pelvic floor dysfunction can also manifest as chronic lower back or abdominal pain, especially when other potential causes (like injury or muscle strain) have been ruled out. Because the pelvic floor muscles are interconnected with the muscles in your lower back and abdomen, any dysfunction can cause tension and discomfort in these areas.
Many women may not immediately associate their back or abdominal pain with pelvic floor issues, often assuming the pain is due to poor posture or normal muscle fatigue. However, chronic or unexplained pain in these regions may be a sign that your pelvic floor muscles are struggling to support your pelvic organs properly.
If you’re experiencing any of the signs mentioned earlier—whether it’s leaking urine during a laugh, feeling pressure in your pelvis, or dealing with lower back pain that you can’t quite explain—it’s essential to seek medical advice. While it may feel tempting to brush these symptoms aside as “just part of getting older” or something that will resolve on its own, these are often early indicators of pelvic floor dysfunction that can worsen over time if left untreated.
The good news is that pelvic floor disorders are highly treatable, especially when addressed early. Seeking help from a urogynaecologist can lead to effective treatment options, whether through pelvic floor therapy, lifestyle modifications, medications, or in more severe cases, surgical intervention. Early intervention not only helps manage the symptoms but can prevent further complications and help you regain control over your overall health and well-being.
Opening up about pelvic floor issues can feel awkward or uncomfortable, but it’s important to remember that your doctor is there to help, and these are common issues they address regularly. Here’s how you can begin the conversation with your urogynaecologist:
Once you’ve identified the signs of a pelvic floor disorder, the next step is exploring treatment options. The good news is that pelvic floor disorders (PFDs) are highly treatable and the range of available treatments can be tailored to your individual needs. From non-invasive therapies to more advanced surgical interventions, treatment plans are designed to address the specific symptoms you’re experiencing and the underlying causes of your pelvic floor dysfunction.
One of the most common and effective treatments for PFDs is pelvic floor physical therapy [6]. This specialised therapy focuses on strengthening or relaxing the pelvic floor muscles, depending on your condition. Although watching videos etc can sometimes be helpful, the connection between the brain and pelvic floor muscles can sometimes be difficult for women to establish reliably. A physical therapist trained in pelvic health will guide you through exercises like Kegels, which target the pelvic muscles and help improve control over bladder and bowel function. They may also use techniques such as biofeedback, electrical stimulation, or manual therapy to enhance muscle coordination and relieve pain.
Pelvic floor therapy is particularly effective for women with stress incontinence, pelvic organ prolapse, or dyspareunia (painful intercourse). It is a non-invasive option that can yield significant improvements with consistent practice and professional guidance.

For many women, making lifestyle changes can greatly improve pelvic floor health. Maintaining a healthy weight, for instance, reduces the strain on the pelvic muscles, especially in women who are overweight or obese. Adopting a fibre-rich diet can help manage constipation, which is a common cause of pelvic floor strain. Avoiding heavy lifting or learning proper techniques to minimise pressure on the pelvic muscles can also prevent further damage.
In addition to dietary and activity modifications, practising good posture and engaging in pelvic floor-friendly exercises (such as low-impact activities like walking, swimming or yoga) can help prevent symptoms from worsening.
In some cases, medications may be prescribed to manage symptoms of pelvic floor disorders. For instance, women with overactive bladder or urge incontinence may benefit from bladder relaxants that help reduce the urgency and frequency of urination [7]. Hormonal treatments, such as topical oestrogen, can also be useful, particularly for postmenopausal women whose symptoms are linked to hormonal changes affecting pelvic tissue strength and elasticity.
These medications can offer relief, but they are often used in combination with other treatments, such as pelvic floor therapy, to address the root cause of the dysfunction.
Vaginal pessaries can be particularly helpful for women who are experiencing bothersome pelvic organ prolapse – they are inserted into one’s vagina and act as mechanical support to alleviate symptoms of pelvic organ prolapse(without the need for surgery) and do not interfere with one’s daily routines. These come in many different shapes and sizes and fitting is done by a trained healthcare professional. Women can be taught how to self-manage and incorporate these to complement various activities/ exercises they may engage in as part of their lifestyle.
For women with more severe cases of pelvic organ prolapse or incontinence – surgery may be necessary. Surgical options vary based on the type and severity of the pelvic floor disorder. Common surgeries include sling procedures to support the bladder [8], colporrhaphy to repair weakened vaginal walls [9] or hysterectomy in extreme cases of uterine prolapse.
Surgery is typically reserved for when non-invasive treatments have not been effective. The decision to undergo surgery should be made after careful discussion with your healthcare provider. While surgery can offer a more permanent solution to severe PFDs, it’s important to weigh the risks and recovery time involved.
It’s important to remember that no two pelvic floor disorder cases are the same. The treatment that works for one woman may not be effective for another. This is why personalised care is crucial. Your gynaecologist will develop a treatment plan based on the specific symptoms you’re experiencing, your medical history and your lifestyle.
While pelvic floor disorders (PFDs) are common, there are several steps you can take to help prevent them or reduce the risk of worsening symptoms. Prevention starts with maintaining the health and strength of your pelvic floor muscles, along with making smart lifestyle choices that minimise strain on this crucial part of your body. Here are some practical and effective ways to protect your pelvic health:
One of the simplest yet most effective ways to prevent pelvic floor dysfunction is by incorporating Kegel exercises into your daily routine. Kegels specifically target the pelvic floor muscles, which helps in strengthening them and maintaining their ability to support your pelvic organs.
To perform a Kegel exercise, imagine you’re trying to stop the flow of urine midstream or trying to stop a fart from coming out. Squeeze and hold the muscles for a few seconds, then relax. Repeat this several times a day. The great thing about Kegels is that you can do them anywhere (except whilst on the toilet bowl to avoid confusing your bladder/rectum) —whether you are sitting at your desk or relaxing at home. Over time, consistent practice can reduce your risk of incontinence and pelvic organ prolapse.
By maintaining a healthy weight, you can reduce the strain on your pelvic muscles and improve overall pelvic health. This does not mean you need to aim for rapid weight loss. Instead, focus on sustainable lifestyle changes, such as eating a balanced diet rich in fruits, vegetables and whole grains, and engaging in regular physical activity. Managing your weight not only supports your pelvic floor but also contributes to your overall well-being.
Many women unknowingly strain their pelvic floor when lifting heavy objects, which can lead to dysfunction over time. To protect your pelvic floor, always use proper lifting techniques:
These simple adjustments can make a big difference in protecting your pelvic muscles from unnecessary strain.
Chronic constipation can be a significant contributor to pelvic floor disorders. To avoid this, focus on maintaining good bowel health by:
If constipation is a recurring issue, it’s important to address it early by consulting a relevant specialist and avoid prolonged straining, which can damage the pelvic floor over time.
Engaging in regular physical activity is essential for overall health, but not all exercises are pelvic floor-friendly. High-impact activities like running or heavy weightlifting can sometimes place excessive strain on the pelvic floor. Instead, focus on low-impact exercises that are gentle on your pelvic muscles while still keeping you active.
Swimming, walking and yoga are excellent examples of pelvic floor-friendly exercises that promote overall fitness without placing undue stress on the pelvic region. These activities can help you maintain strong muscles, reduce your risk of injury, and support your pelvic floor’s health.
By incorporating these preventive measures into your lifestyle, you can significantly reduce the risk of developing pelvic floor disorders. Preventing PFDs is all about staying mindful of how you use and care for your body—strengthening your muscles, avoiding unnecessary strain, and making smart choices that support your long-term pelvic health.
Recognising the early signs of a pelvic floor disorder is the first step toward regaining control of your health and well-being. By being aware of the symptoms and seeking medical advice early, you can address these issues before they progress. With proper treatment, whether through pelvic floor therapy, lifestyle changes, or other interventions, it’s entirely possible to manage and even resolve pelvic floor dysfunction.
Remember, you don’t have to live with discomfort, pain or embarrassment. With the right support and care, you can significantly improve your quality of life and enjoy a more active, comfortable, and fulfilling day-to-day routine.
If you’re experiencing any of the signs mentioned in this article, don’t hesitate to reach out. Contact our clinic today to schedule an evaluation and take the next step toward restoring your pelvic health. We are here to help answer your questions and guide you on your journey to wellness.
Your first gynaecological visit is an essential step in taking charge of your reproductive health. While it’s normal to feel a bit anxious or unsure, understanding the significance of this visit can help you approach it with confidence. This isn’t just a routine check-up; it’s an opportunity to establish a baseline for your health, address any questions or concerns, and build a relationship with a healthcare provider who can support you through all stages of life.
Many young women worry about what will happen during the visit, often fearing pain, discomfort, or embarrassment. However, it’s important to know that gynaecologists are trained professionals who prioritise your comfort. Your first visit may involve a conversation about your health history, menstrual cycle, and any specific concerns you have. Physical exams, if necessary, are usually straightforward and will be explained to you every step of the way.
Remember, this visit is a normal and essential part of women’s healthcare, regardless of whether you’re experiencing issues or are sexually active. Starting early with regular gynaecological visits can help you stay informed and proactive about your health. By making this first appointment, you’re taking a positive step toward a lifetime of well-being.
In this article, we will discuss why you shouldn’t delay your first gynaecological visit, what to expect during the exam, how to prepare, and what questions to ask, so you can approach your first visit with confidence and ease.

Delaying your first gynaecological appointment can have significant implications for your long-term health. Early gynaecological care is essential not only for addressing immediate concerns but also for establishing a foundation of proactive and preventive health practices that can benefit you throughout your life.
Despite the importance of early care, many young women delay their first gynaecological visit for various reasons. One of the most common reasons is fear or anxiety about the unknown—worrying that the visit will be painful, embarrassing, or uncomfortable. There’s also a widespread misconception that gynaecological care is only necessary once a woman becomes sexually active, leading some to postpone their first visit unnecessarily.
Others might delay because they feel that their symptoms are not serious enough to warrant a visit or because they feel embarrassed discussing intimate health issues with a doctor. Additionally, cultural or familial beliefs may play a role in postponing the first appointment, as some young women may receive mixed messages about the importance of reproductive health care.
It’s crucial to recognise that these fears and misconceptions, while common, shouldn’t prevent you from taking charge of your health. Gynaecologists are trained to handle these situations with care and professionalism, and they ensure that you feel comfortable and informed throughout the process.
Early gynaecological care is a vital part of maintaining your overall health and well-being. A gynaecologist can help you manage various aspects of reproductive health, from understanding your menstrual cycle to discussing birth control options and screening for potential health issues. Starting these visits early allows your gynaecologist to identify any underlying conditions that may not present symptoms immediately but could lead to complications if left untreated.
For instance, conditions like polycystic ovary syndrome (PCOS), endometriosis, or sexually transmitted infections (STIs) might not always have obvious symptoms in their early stages but can impact your reproductive health if not addressed promptly. Regular visits also provide an opportunity for cancer screenings, such as Pap smears and HPV tests, which can detect precancerous changes in the cervix long before they develop into more serious conditions.
Moreover, early visits also provide an opportunity to establish a relationship with your gynaecologist, which can make it easier to discuss sensitive topics openly. This trust and familiarity can make future visits less intimidating and more productive, as your gynaecologist becomes a trusted partner in your health care.
Additionally, early gynaecological care helps you establish healthy habits that can support your overall well-being. Whether it’s understanding how to manage your menstrual cycle, learning about safe sexual practices, or exploring contraception options, these early conversations lay the groundwork for a lifetime of informed health decisions.
Deciding when to schedule your first gynaecological visit is a crucial step in taking charge of your reproductive health. While the timing can vary depending on individual circumstances, there are general guidelines and recommendations from leading health organizations that can help you determine the right time for your first appointment.
The American College of Obstetricians and Gynaecologists (ACOG) [1] recommends that young women schedule their first gynaecological visit between the ages of 13 and 15. This initial visit often serves as an introductory meeting rather than a full physical exam, which allows you to build a rapport with your gynaecologist and gain valuable information about your reproductive health. At this age, the focus is typically on education and guidance, addressing topics such as menstrual health, sexual development, and preventive care.
ACOG’s recommendation for the first visit between ages 13 and 15 is widely supported by other health organisations, including the American Academy of Pediatrics (AAP) [2]. These organisations emphasise the importance of early education and preventive care as a foundation for lifelong reproductive health.
In some cases, parents or guardians might hesitate to schedule a gynaecological visit for their adolescent daughters, fearing that it implies sexual activity. However, these early visits are not necessarily focused on sexual health alone; they are a key part of overall health care, providing a safe space for young women to learn about their bodies and ask questions in a confidential setting.
While the age guidelines provide a general framework, there are specific signs and circumstances that indicate it’s time to book your first gynaecological appointment:
Your first gynaecological exam can feel daunting, but understanding what to expect can help ease any anxiety and ensure you feel more comfortable during the visit. A gynaecological exam is a routine procedure designed to assess your reproductive health and provide you with the care and information you need. Here’s a detailed walk-through of what typically happens during the exam, so you can be prepared and informed.
When you arrive for your appointment, you’ll first check in at the reception and may be asked to fill out some forms regarding your medical history. This information is crucial for your gynaecologist to understand your overall health and any specific concerns you might have.
A nurse or medical assistant will likely measure your weight, height, and blood pressure. The exam usually starts with a general discussion about your health. Your gynaecologist may ask about your menstrual cycle, sexual activity, any symptoms or concerns, and your medical and family history. This conversation is an important part of the exam, as it helps your gynaecologist provide personalised care tailored to your needs. You’ll then be asked to get changed in privacy for the physical examination. Your gynaecologist will inform you before entering the room to ensure your privacy and comfort.
It is understandable that you might feel the need to groom or shave before your gynaecological visit (or even postpone it until the aforementioned is done), but it’s actually not necessary. Your gynaecologist is primarily focused on your health and well-being, and they won’t be concerned about grooming.
A typical gynaecological exam is composed of several key components, each serving a specific purpose:

The entire gynaecological visit, including the time spent discussing your health, typically lasts between 30 minutes to an hour. The actual physical exam portion may only take about 10 to 15 minutes. The length of the visit can vary depending on whether it’s your first appointment, the complexity of your health history, and any specific concerns you have.
Your gynaecologist will also take time at the end of the exam to discuss any findings, answer your questions, and guide you on your next steps, such as when to return for follow-up visits or how to manage any health issues that were identified.
While your first gynaecological exam might feel a bit intimidating, it’s an essential step in maintaining your reproductive health. Knowing what to expect can help you feel more at ease and ensure that you’re prepared to take full advantage of the care and advice your gynaecologist provides.
Your first gynaecological visit is not just about undergoing a physical exam—it’s also an opportunity to ask questions and gain a deeper understanding of your reproductive health. Preparing a list of questions beforehand can help ensure that you leave the appointment feeling informed and confident about your health. Here are some essential questions every young woman should consider asking during her gynaecological visit.
Understanding what’s typical for your menstrual cycle is key to recognising when something might be off. Ask your gynaecologist about what constitutes a normal cycle, and discuss any irregularities, such as heavy bleeding, severe cramps, or missed periods. This can help you determine if your experiences are within the normal range or if further investigation is needed.
If you experience significant discomfort during your periods, your gynaecologist can provide strategies for managing pain and premenstrual syndrome (PMS). This may include lifestyle changes, over-the-counter medications, or hormonal treatments. Discussing these options can improve your quality of life and help you manage your menstrual cycle more comfortably.
Contraception is a critical aspect of reproductive health, and there are many options available, each with its own benefits and potential side effects. Your gynaecologist can help you understand the various methods, including birth control pills, intrauterine devices (IUDs), implants, patches, and more. Together, you can discuss your lifestyle, health conditions, and preferences to find the method that best suits your needs.
If you’re sexually active, it’s essential to understand how to protect yourself from STIs and what steps to take if you think you’ve been exposed. Ask your gynaecologist about routine STI screening, symptoms to watch for, and the best practices for prevention. Open communication about your sexual health is crucial for maintaining your overall well-being.
Changes in vaginal discharge, odour, or itching can be concerning and might indicate an infection or other health issue. Discuss with your gynaecologist what’s normal and when you should seek medical advice. Understanding your body’s signals is vital for catching potential problems early.
Certain vaccines, like the human papillomavirus (HPV) vaccine [5], are important for preventing infections that can lead to more serious health issues, such as cervical cancer. Ask your gynaecologist about recommended vaccines for your age and health status.
Your gynaecologist can provide guidance on how diet, exercise, and stress management can impact your reproductive health. This is a great time to discuss any concerns you have about your lifestyle and receive personalised advice.
During your visit, it’s important to cover a range of topics that are relevant to your overall reproductive health. These include:
One of the most important aspects of your gynaecological care is establishing open and honest communication with your gynaecologist. This relationship is built on trust, and being transparent about your concerns, habits, and lifestyle will allow your gynaecologist to provide the best possible care. Remember, your gynaecologist is a trained professional who is there to support your health, not to judge you. The more open you are, the more personalised and effective your care will be.
Don’t be afraid to ask questions, no matter how small or personal they may seem. Your gynaecologist has heard it all and is there to help you navigate your reproductive health with confidence and knowledge.
Your first gynaecological visit is more than just a medical appointment; it’s a crucial step in taking control of your reproductive health and well-being. By understanding the importance of this visit and what it entails, you’re empowering yourself with the knowledge and confidence needed to make informed decisions about your body.
Regular gynaecological care is a cornerstone of preventive health, which can help you stay ahead of potential issues and ensure that you receive the guidance and support you need at every stage of life. From menstrual health to contraception options and beyond, these visits provide the foundation for a lifetime of proactive care.
If you haven’t scheduled your first gynaecological visit yet, now is the time to do so. Don’t let fear or uncertainty hold you back from taking this important step. Embrace the journey of caring for your reproductive health, and make your well-being a priority today.

As its name suggests, hormone replacement therapy (HRT) replaces the hormones that decline during the perimenopausal and menopausal periods. But what is menopause, and how does it impact women’s health? What is the significance of hormone replacement therapy (HRT), and is it even necessary? In this article, we delve into the world of menopause and HRT, giving you the knowledge to help you make the right decision.
Menopause is a natural biological process that marks the end of a woman’s reproductive years. It typically occurs in middle age, usually in a woman’s late 40s to early 50s, although this varies between individuals. One is deemed to have reached menopause if there is cessation of menstruation (periods) for one year, and women typically undergo a perimenopausal transition prior to that. This whole process may also be associated with a range of physical and hormonal changes in a woman’s body.
The main hallmark of menopause is a decline in the production of certain hormones, particularly estrogen and progesterone, by the ovaries. This hormonal shift can lead to a variety of physical and emotional symptoms.
Common perimenopausal/ menopausal symptoms include:
If you are experiencing any of the symptoms stated above, you are not alone, as this is a physiological process that every woman needs to go through eventually. Make an appointment with your gynaecologist to understand what you are going through and learn how to navigate the next chapter of your life, especially if you find that your quality of life is being adversely affected.

Hormone replacement therapy is used to alleviate the symptoms of menopause by effectively replacing the hormones (oestrogen and progesterone), which levels decline during the perimenopausal/menopause period.
There are different types of hormone therapy, these are:

As much as hormone replacement therapy (HRT) can offer benefits, there can be potential risks/side effects involved, which also depends on the type of HRT, duration of use, individual’s health profile and other considerations.
The decision to use HRT should be individualised, taking into account a woman’s medical history, age, risk factors, and the severity of her menopausal symptoms. It’s essential to have a thorough discussion with your gynaecologists to weigh the potential benefits and risks. The optimal duration of HRT also varies from person to person. Regular follow-up with your gynaecologist is crucial to monitor the effects of HRT and adjust the treatment plan as needed.

Hormone replacement therapy is not for everyone. There are also several contraindications to consider before even considering this treatment. This is why a thorough consultation with a specialist is essential if you plan on going on hormone replacement therapy.
There are several alternatives to Hormone Replacement Therapy (HRT) for managing the symptoms of perimenopause and menopause. The choice of alternatives depends on an individual’s specific symptoms, preferences, and medical history. Here are some common alternatives to HRT:

Before considering HRT, there are several important factors and considerations.
The decision to use HRT should be based on an individualised assessment of benefits and risks in consultation with a healthcare provider. HRT is not a one-size-fits-all solution. It should be tailored to an individual’s specific needs, considering their medical history, health profile, and menopausal symptoms – i.e. its use should be informed, individualised, and closely monitored. Ultimately, the decision to use HRT is a personal one that should be made in collaboration with your gynaecologist to optimise health and well-being during and after menopause.

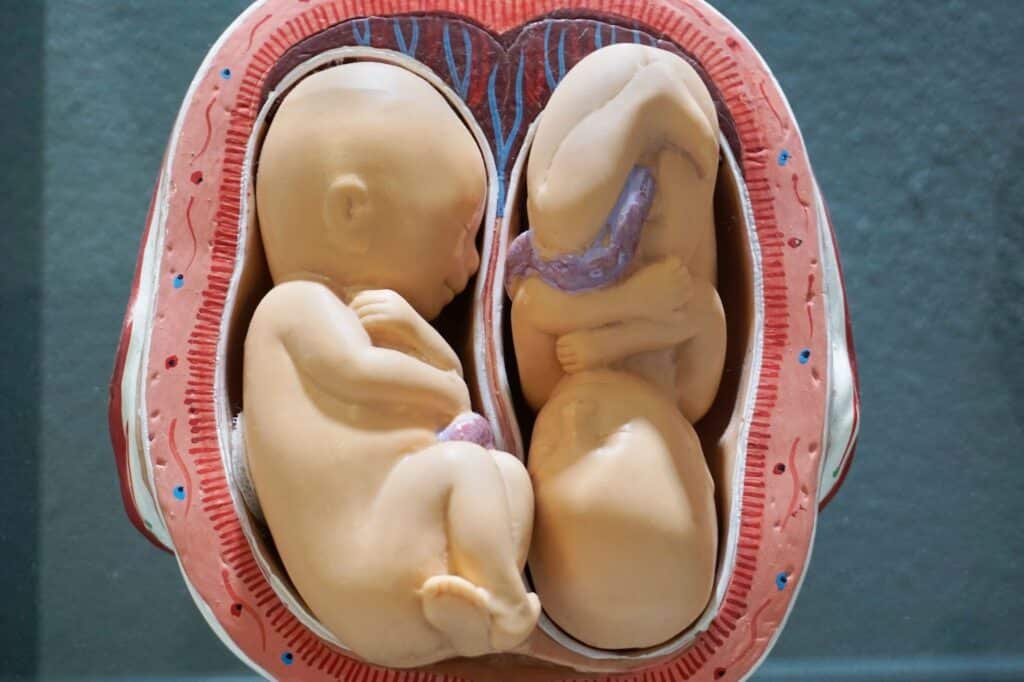
A high-risk pregnancy can be challenging for expectant mothers and their healthcare teams, as it comes with an elevated probability of complications that can impact both the mother and the developing foetus.
This article will discuss what constitutes a high-risk pregnancy and the factors behind it. From maternal age and multiple pregnancies to pre-existing medical conditions, gestational complications, and a history of previous issues, we’ll explore the various elements that healthcare professionals consider when assessing pregnancy risk.
A high-risk pregnancy, also known as a high-risk gestation or high-risk obstetric pregnancy, is a pregnancy that has a higher likelihood of complications for the mother, the foetus, or both compared to a typical pregnancy.
Various factors can contribute to a pregnancy being categorised as high-risk, including:

If you have a high-risk pregnancy, it is crucial for you to consult a highly professional obstetrician and gynaecologist and to ensure regular monitoring throughout your pregnancy. This approach greatly enhances the likelihood of a healthy pregnancy and safe delivery for you and your baby.
Prenatal care is essential for the health and well-being of expectant mothers and their developing babies. Regular prenatal care involves a series of medical check-ups, screenings, and guidance throughout the pregnancy. Here’s why prenatal care is so important:

Managing a high-risk pregnancy requires close collaboration between you, your healthcare team, and, sometimes, specialists. Here are some key steps to help manage a high-risk pregnancy:

Remember that each high-risk pregnancy is unique, and the management plan will be tailored to your circumstances. Always consult with your doctor for guidance and support throughout the pregnancy. The goal is to optimise the health and safety of both you and your baby.
In high-risk pregnancies, some essential preparations should be made for the delivery to ensure the safety and well-being of both the mother and the baby. These preparations include:
The goal of managing high-risk pregnancies is mitigating risks by optimising maternal and foetal health. This is done through medical interventions, lifestyle modifications, or both. In conclusion, it is safe to say that the management of high-risk pregnancies requires a team approach, personalised care, and a focus on early detection and intervention.
Work closely with your obstetrician and follow their advice and guidance. This way, you can increase your likelihood of a healthy pregnancy and the birth of a healthy baby.
The myriad of birth control methods can sometimes prove confusing for many especially when considering different lifestyle factors. Contraception, commonly known as birth control, comes in various forms that are used to prevent unplanned or unwanted pregnancies. Before we learn about how birth control works, it is important to understand that birth control is only efficient when used properly, correctly, and consistently. A poor lapse of judgement may not only result in an unplanned or unwanted pregnancy but may also bring about a sexually transmitted infection (STI).
In this article, we will delve into:
There are many different types of birth control methods such as:
These rely on hormones to prevent pregnancy. Routes of administration vary and range from oral tablets, skin patches, vaginal rings, intramuscular injections, contraceptive implants (aka Implanon/Nexplanon), to intrauterine devices.
Types of hormonal birth control include:
Some of these methods also serve dual functions such as menstrual regulation and relief of menstrual symptoms which include menstrual cramps/heavy period flow, etc [2].
These methods prevent pregnancies without the use or interference of hormones.
Types of non-hormonal birth control include:

There are strengths and weaknesses for each birth control method. It is important to evaluate them to ensure you are making an informed decision.
| Birth control method | Effectiveness | Pros | Cons |
|---|---|---|---|
| Birth control pills | Perfect use: 99%
Typical use: 91% |
Oral administration
Helps in menstrual regulation, relief of menstrual cramps, and heavy flow
Short-term and no delay in the return of fertility after stopping |
Must be taken at the same time daily
Side effects include headaches, nausea, bloating, breast tenderness, etc. (usually improves after first few months) |
| IUCD/IUD | 99% | User independent; Mirena IUD also helps in the relief of menstrual cramps and heavy flow
Lasts for 5 years (but removable prior to that if keen for pregnancy, with no delay in the return of fertility) |
Invasive – needs to be placed inside the uterine cavity
Commonly results in erratic periods, and prolonged/unscheduled bleeding especially in the first 6 months Small risk of infection |
| Birth control patch | Perfect use: 99%
Typical use: 91% |
Skin patch administration
Helps in menstrual regulation, relief of menstrual cramps, and heavy flow
Short-term and no delay in the return of fertility after stopping |
Must be changed on a weekly basis
Side effects include skin irritation, headaches, nausea, bloating, breast tenderness, etc. (usually improves after first few months) |
| Birth control implant | 99% | User independent
Helps in the relief of menstrual cramps and heavy flow Lasts for 3 years (but removable prior to that if keen for pregnancy, with no delay in the return of fertility) |
Invasive – needs to be inserted underneath the skin
Commonly results in irregular periods and prolonged/unscheduled bleeding especially in the first 6 months |
| Birth control injections | Perfect use: 99%
Typical use: 94% |
User independent (during 3 months post-administration)
Helps in the relief of menstrual cramps and heavy flow |
Commonly results in irregular periods and prolonged/unscheduled bleeding
Delay in the return of period and fertility after cessation Associated with weight gain and decrease in bone mineral density |
| Condoms | Perfect use: 95%
Typical use: 70% |
No serious side effects
Widely available Helps protect against sexually transmitted infections (STIs) |
May slip off/break during intercourse
Penis must be withdrawn immediately after ejaculation |
| Vaginal ring | Perfect use: 99%
Typical use: 91% |
Helps in menstrual regulation, relief of menstrual cramps, and heavy flow
Short-term and no delay in the return of fertility after stopping |
Must be changed on a weekly basis
Side effects include vaginal discharge, headaches, nausea, bloating, breast tenderness, etc. (usually improves after first few months) |
| Spermicide | Perfect use: 80%
Typical use: 70% |
No severe side effects
Widely available |
Low efficacy when used alone
Usually needs to be combined with other methods e.g., condoms/diaphragm |
| Diaphragm | Perfect use: 95%
Typical use: 70% |
No severe side effects | Needs to be fitted correctly (every woman’s cervix is slightly different)
Must be combined with other methods e.g., spermicide |
| Fertility awareness/ Natural family planning | Perfect use: 99%
Typical use: 75% |
No severe side effect
Can be used for pregnancy planning |
Close tracking is needed to understand one’s body clock (at least a few months to learn) |
| Morning after pill | 98% (if administered within a certain timeframe) | Can be used as a last resort should one’s regular contraceptive method fail | Not suitable as regular/long-term contraception
Must be administered within a certain timeframe Side effects include nausea/vomiting, dizziness, unscheduled bleeding etc. |
| Abstinence | 100% | High effectiveness | May not suit everybody |
| Tubal ligation | 99.5% | Highest success rates in preventing pregnancy
Does not affect periods |
Invasive – requires day surgery with associated surgical/anaesthetic risks
Permanent/irreversible |
| Vasectomy | 99.8% | Highest success rates in preventing pregnancy | Invasive – requires day surgery with associated surgical/anaesthetic risks
Requires follow-up sperm test to show the absence of sperm in semen Permanent/irreversible |
These methods have varying effectiveness and different pros and cons when it comes to preventing pregnancy, however, not all birth control methods are created equal.
Of note, only barrier contraceptives can prevent pregnancies and sexually transmitted infections (STIs) – that means if you are on another form of birth control e.g., birth control pills and also wish to protect yourself against STIs, you should combine them with the use of condoms during every sexual encounter.

“So, what is the best birth control for me?” This answer will vary on a case-by-case basis. The decision will boil down to which factor you deem most important. In fact, your ideal birth control method may differ depending on which part of your life you are in.
There are several things to consider before deciding on the most effective birth control method, including:
Bear in mind that these factors must be considered in relation to your lifestyle and whether you are able to commit to the responsibilities necessary for the birth control method to be effective.
| Factors | Birth control method |
|---|---|
| Comfort: “I want birth control that doesn’t impede my sexual experience. I also have a monogamous relationship and sex is an important aspect of our relationship.” |
Birth control pills
Birth control patch/skin patch Vaginal ring IUCD (Mirena or copper) Contraception implant (Implanon/Nexplanon) Surgery (tubal ligation/vasectomy) |
| Lifespan:
“I want a contraceptive that lasts long and requires minimum management.” |
IUCD (Mirena or copper) – 5 years
Contraception implant (Implanon/Nexplanon) – 3 years Surgery (tubal ligation/vasectomy) – forever Abstinence – as long as you can manage |
| Affordability:
“I want a contraceptive that is cheap and will still keep me safe.” |
Condoms
Diaphragm + spermicide Fertility awareness/natural family planning Abstinence |
| Protection against STI:
“I want a contraceptive that prevents pregnancy and protects me from STIs as I have multiple partners.” |
Condoms |
| Convenience:
“I want a birth control method that doesn’t involve visiting a health care provider.” |
Condoms
Abstinence Fertility awareness/natural family planning |
| Side effects:
“I want a birth control method that doesn’t affect my hormonal cycle.” |
Non-hormonal methods of contraception |
No. The pull-out method, also known as the withdrawal method or coitus interruptus, involves pulling the penis out before ejaculation occurs. It is not an effective form of birth control as sperm exists in pre-ejaculate [3,4]. Pre-ejaculate is released during arousal and may contain sperm due to previous sessions of ejaculation. This sperm can still result in pregnancy, in fact, statistics have shown that 1 in 5 couples who use the pull-out method will still end up falling pregnant [5].

There are two main types of birth control pills in Singapore, these are prescription-only and include the following:
In general, if you are thinking about going on contraception, do make an appointment to see an obstetrician who will be able to tailor and individualise your birth control options according to your needs – there is no one-size-fits-all.
Exercise is vital for a healthy life, pregnancy is no exception. Exercise can help maintain or improve your body’s strength, flexibility, and even boost your mood (which might be a little sensitive during pregnancy). But the age-old question remains: is exercise safe during pregnancy?
In this article, we will explore the safety of exercise during pregnancy, the benefits of exercise during pregnancy, pregnancy-safe exercises, and exercises that encourage an easy birth.
In short, it depends. There are various factors that may prevent some women from safely exercising during pregnancy, which include:
With these in mind, it is essential to check with your obstetrician and obtain clearance before you commence exercising.
For most women however, exercise during pregnancy is safe; the bottom line is – if you are healthy and your pregnancy is normal/low risk, it is safe to exercise and you should exercise to maintain your physical stamina throughout your pregnancy journey [1-4].

During pregnancy, your body goes through a plethora of changes such as a change in the centre of gravity, backaches, bloating, constipation, and weight gain. Exercise has been shown to be incredibly beneficial during pregnancy [5].
Exercise during pregnancy has been found [3] to promote the following:

Once you have gotten the go-ahead from your obstetrician, you can start exercising in any month of your pregnancy. How to kick start exercising during pregnancy depends on your fitness level prior to pregnancy; if you led a largely sedentary lifestyle prior to pregnancy, start low and go slow – begin by incorporating just 10 minutes of light exercise a day, this may include walking, yoga, stretching, or swimming.
If you were generally fit and exercised regularly before conceiving, you will be able to keep to your usual exercise routine barring physical impediments e.g., as your belly grows bigger. Ultimately, you know your body best and it is important to listen to your body and the advice of your doctor.
Depending on your fitness level, the following low-impact exercises are considered safe for pregnancy:
Exercises not considered safe for pregnancy are:
High-impact exercises with risks of direct or indirect trauma to your belly are a definite no-no during pregnancy. Additionally, exercises or activities that involve exposure to high temperatures like hot yoga, hot pilates, sauna, and hot tubs are also generally not advisable during pregnancy [6].
An easy birth or delivery is one of the most important aspects of giving birth. Fortunately, there are several types of exercises that encourage an easy birth, these include:
In conclusion, for most women, exercise during pregnancy is safe and beneficial. Consult with your obstetrician to find out what is suitable for you, listen to your body, and listen to your doctor.
Pelvic floor disorders are a group of conditions that affect the muscles, ligaments, nerves and connective tissue in the pelvic region. These disorders can affect both men and women, and include conditions such as pelvic organ prolapse and urinary/ bowel dysfunction such as urinary incontinence.
Pelvic floor disorders can have a significant impact on a person’s quality of life and require medical attention for prompt diagnosis and proper treatment.
Giving birth can indeed put significant strain on your pelvic floor muscles, which in turn leads to damage and weakness.
The process of childbirth, particularly vaginal delivery, can have a sizable impact on the muscles, ligaments, nerves and connective tissue in the pelvis.
Risk factors that put women at higher risk of pelvic floor dysfunction include:
Fortunately, not every woman who has undergone childbirth will go on to develop pelvic floor disorders/weakness; pelvic floor exercises (Kegels) can improve the state of the pelvic floor following delivery, although in some women, the pelvic floor weakness can persist and ultimately require treatment to improve their quality of life.
Although there have been studies[1] that show a lower incidence of pelvic organ prolapse for women who delivered exclusively through caesarean sections versus women who delivered vaginally, having a caesarean section does not guarantee that you will never suffer from pelvic floor weakness.
One also needs to take into account the strain on the pelvic floor muscles over the 9-month pregnancy journey, the numerous surgical risks of having a caesarean section, including:
It is recommended that the decision on one’s mode of delivery (whether via vaginal birth or caesarean section) be individualised and discussed with your obstetrician, taking into account both maternal and fetal factors.
The pelvic floor muscles can return to supporting normal pelvic functions after birth, but this depends on a number of factors such as:
Physical therapy and exercises specifically targeting the pelvic floor are helpful[2] in strengthening the weakened pelvic floor muscles following childbirth, although it is important to note that this takes time and consistent effort.
If you feel that you may be suffering from a weak pelvic floor, you should seek guidance from a healthcare professional who specializes in pelvic floor rehabilitation.
Having a strong pelvic floor may not specifically help you with the childbirth process, but can certainly counter the strain exerted on your pelvic floor from the growing baby throughout the pregnancy, and minimize the risk of pelvic floor damage sustained during childbirth – this translates to you having a lower risk of experiencing urinary/faecal incontinence as well as pelvic organ prolapse both in the short- and long-term.
Symptoms of a weak pelvic floor can range from woman to woman – in some cases, it can manifest in involuntary urinary/faecal leakage, feeling pelvic heaviness or even a lump in your vagina.
The good news is that most of these symptoms will improve and/or resolve with time so there is no need to panic – just as you took 9 months to nurture a baby, do remember that it is equally important to give your body some time and breathing space to go back to its pre-pregnancy state.
Do engage your pelvic floor muscles regularly by doing Kegel exercises, and if you still feel that you may be suffering from a weak pelvic floor after some time, you should seek guidance from a healthcare professional who specializes in pelvic floor rehabilitation who can do a proper pelvic examination and determine the degree of pelvic floor dysfunction, if any.
Do you have any questions about pelvic floor dysfunction? Feel free to contact me.
Gestational diabetes mellitus, or GDM for short, is a type of diabetes that occurs during pregnancy and typically diagnosed during the 2nd half of your pregnancy via an oral glucose tolerance test (OGTT).
The OGTT is a series of blood tests (usually done between 24 to 28 weeks of pregnancy) that is first performed after you have fasted, and is then repeated 1 and 2 hours after you drink a sweet drink with a fixed sugar content.
The diagnosis of GDM is ascertained if your blood sugar levels remain persistently high in any of your serial blood tests. Thankfully, the majority of pregnant women who get diagnosed with GDM do have resolution of this condition after delivery.
Risk factors of GDM include;
Although having one or more of these risk factors does not necessarily mean that a woman will develop GDM, this condition remains very common in Singapore, with 1 in 5
[1] pregnant women being afflicted by it.
Hence, it is common practice in Singapore to universally screen for GDM in all pregnant mothers so that the condition can be diagnosed and managed on a timely basis.
Under normal circumstances, insulin (a hormone) is made by the pancreas and utilizes blood sugar for the body.
During pregnancy, your body undergoes some physiological changes that result in insulin resistance – this causes your cells to be less effective in using insulin. This in turn leads to high blood sugar levels.
Majority of pregnant women with GDM have no specific symptoms or warning signs of their condition, which makes universal screening all the more important.
Occasionally, if the blood sugar levels are extremely high, some women may experience increased thirst and frequent urination, fatigue and hunger – however, some of these may overlap with common symptoms that pregnant women experience in general, so it is vital to check in with your obstetrician if you are experiencing any of these.
Majority of women with GDM will go on to have successful pregnancies with healthy babies, particularly if their GDM is well controlled. Good control of GDM is typically achieved by:
It is important to keep blood sugar levels within a target range (this applies to both pre- and post-meal readings) to prevent high blood sugar levels to minimize the risk of pregnancy complications, and you will likely require more frequent antenatal visits and ultrasound scans to check on the well-being of the baby.
Whilst the majority of pregnant women will be able to control their GDM simply through the combination of healthy eating and exercise, some women may require additional help in the form of medication.
Depending on the severity of the condition, this may require the input of an endocrinologist (diabetes specialist) for titration of either oral medications or insulin injections to keep your BSP values stable – the medications prescribed will be safe for your pregnancy and it is extremely important to be compliant with the outlined treatment plan to ensure good pregnancy outcomes.
Poorly controlled GDM can expose the mother and child to pregnancy complications, such as;
Even though GDM resolves in most women following childbirth, women with a history of GDM still remain at an overall higher risk of developing type 2 diabetes mellitus later on in life as compared to the baseline population, and it is advisable you keep to a healthy lifestyle with regular screening for diabetes as you get older. It may also be necessary for you to be screened for diabetes at the start of your subsequent pregnancies.
You may not be able to prevent GDM if you have a genetic predisposition to it, but ways to reduce the risk of developing GDM include the following:
Do you have any questions regarding your pregnancy? Feel free to contact me.
https://www.healthhub.sg/live-healthy/1606/gestational-diabetes-what-you-need-to-know
A urinary tract infection, or UTI for short, refers to an infection that can occur in any part of the urinary system – this includes the kidneys, ureters (pipes that carry urine from the kidneys to the bladder), bladder and urethra (tube through which urine leaves the body).
UTIs are typically caused by bacteria which enters the urinary system through the urethra and travels to the bladder. They are much more common in women than in men, owing to their shorter urethra (this makes it easier for the bacteria to enter and reach the bladder to result in cystitis i.e. bladder infection).
There are several risk factors that increase a person’s likelihood of developing a urinary tract infection (UTI). Some of the most common risk factors include:

Symptoms of a UTI may include;
In severe cases, fever, nausea, or vomiting may occur; some may experience either a left or right flank pain if the UTI has progressed upwards to infect the kidney.
It is important to note that you may experience one or more of the fore-mentioned symptoms, and not necessarily the full spectrum. Different UTI episodes in the same person may also present in different ways.
In some cases, people with UTIs may not present with any symptoms and are incidentally picked up when urine tests are done for other reasons e.g. during a routine health screening.
Very mild UTIs may go away on its own, particularly if you are able to recognise it early and adopt some measures e.g. drinking more water to flush out the urinary system, or taking certain over-the-counter urinary alkaliniser, which works by raising the pH of urine.
However, once full-blown, a UTI is unlikely going to resolve on its own without treatment.
If you suspect that you may be having a UTI, you should visit your doctor as soon as possible to get some tests done. This is to reduce the risk of the UTI worsening and leading to a kidney infection, which can potentially make you extremely sick or even be life-threatening in some cases.
Your doctor will usually arrange for a urine microscopy (to check the number of red and white blood cells in your urine sample that may suggest the presence of a UTI) and a formal urine culture (to determine what bacteria is causing your UTI and which antibiotics is the most effective treatment for it).
It is not advisable to self medicate; if you have been given antibiotics by your doctor for your UTI, it is important to complete the course of antibiotics even if you feel better before the course is over, as incomplete therapy can encourage the emergence of multiresistant bacteria and make future UTIs challenging to treat.
The American Urological Association[1] defines recurrent UTIs as two episodes of acute bacterial cystitis within six months or three episodes within one year.
These definitions typically consider these episodes to be culture proven and separate infections with the resolution of symptoms between episodes; this is because the accuracy of clinical diagnoses can vary considerably.
If you have recurrent UTIs, it is best to consult a urologist or a urogynaecologist (if you are a female) who will need to take a detailed history and perform physical examination/ further investigations to delineate the possible causes of your recurrent UTIs.
Further investigations may include;
Depending on the findings, there are some measures that may be suggested to reduce the risk of recurrent UTIs – these include:
Do you have any questions regarding UTIs? Feel free to contact me.
Vaginal laxity is a poorly understood symptom of pelvic floor dysfunction, yet comes with a significant degree of bother for women with potential impact on interpersonal relationships and sexual intercourse.
Case in point – a study published in the International Urogynaecology Journal[1] stated that the associated bother of vaginal laxity was almost as high as the bother associated with conventional prolapse symptoms.
Although there is no international consensus on the exact definition of vaginal laxity, it is colloquially known as a sensation of vaginal “looseness”. Vaginal laxity can occur together with pelvic organ prolapse, whereby a woman’s pelvic organs (i.e. the bladder, uterus or rectum) droop into and/or beyond the vagina, but can also occur in isolation. A recent research article in the Journal of Sexual Medicine[2] found no correlation between vaginal laxity and physical examination findings of pelvic organ prolapse or sexual function.
Yet another study[3] showed decreasing prevalence of vaginal laxity with age, whilst symptoms of pelvic organ prolapse increase with age, concluding that vaginal laxity was not an early symptom of pelvic organ prolapse. These findings reveal the need for better quantification of vaginal laxity.
Given the “iffy” nature of vaginal laxity and its lack of standardized definition or assessment tool, it can be hard to delineate the causes of vaginal laxity. Contributory risk factors may include;
Some women may report a persistent feeling of “looseness” in their vagina, which may be associated with discomfort, heaviness, a dragging sensation or even pain.
These symptoms can prove to be troubling for the woman and may even affect her body perception, self-esteem and ability to derive satisfaction from her intimate, sexual relationships.
The spectrum of symptoms and bother can be quite wide-ranging and vary between women.
Unfortunately, there is no definite way to check for vaginal laxity, and because of the lack of a globally accepted assessment tool for vaginal laxity, your gynaecologist can only check for the presence of pelvic organ prolapse on vaginal examination, which may be poorly correlated to your symptoms as mentioned earlier.
Vaginal relaxation syndrome refers to relaxation of the vaginal walls, and is currently used interchangeably with the term vaginal laxity.
From a physical health perspective, unless it is correlated with findings of pelvic organ prolapse and/or urinary incontinence (due to common shared risk factors), vaginal relaxation syndrome does not pose a threat nor act as a harbinger of medical diseases; however, it may come with significant psychological burden to the woman and her partner, which can be socially debilitating.
Studies showing definitive treatment success for vaginal relaxation syndrome in existing literature remain limited, with small sample sizes of women studied and findings still a mixed bag.
Radiofrequency therapy and laser procedures have come up recently as topics of interest and have been advocated as part of “vaginal rejuvenation” to be a safe, efficacious and non surgical treatment approach[4] for vaginal laxity with high patient satisfaction and minor adverse events.
However, much research is still needed to determine the true effectiveness of “vaginal rejuvenation” on vaginal laxity, the appropriate training, how long the treatment effects can last for, if repeat/maintenance treatment is required and at what intervals, and long-term safety concerns.
In the meantime, Kegel (pelvic floor) exercises is generally a fail-safe way to improve your pelvic floor tone and muscle strength, and should be performed as early as in your antenatal period with long-term incorporation into your daily exercises – as it has certainly been proven to help with both pelvic organ prolapse and urinary incontinence.
Do you have any questions? Feel free to drop me a message!





Aster Gynaecology © | All Rights Reserved.
