Within the realm of women’s health, the terms “fibroids” and “cysts” are often mentioned in passing, and sometimes, occur concurrently. While they may sound similar, fibroids and cysts are entirely different in nature — one is a solid tumour-like growth in the uterus, while the other is a fluid-filled sac that develops in the ovaries.
The confusion often comes from the fact that both can develop silently, without obvious symptoms, or they can cause discomfort, changes in menstrual patterns, and, in some cases, complications.
In this article, we’ll break down everything you need to know about uterine fibroids and ovarian cysts — their differences, symptoms, diagnosis, and treatment options — so that you can make informed decisions about your health. Whether you’re facing a recent diagnosis, dealing with unexplained symptoms, or simply want to be proactive about your gynaecological health, understanding these conditions can empower you to take control of your well-being.
What Are Uterine Fibroids?
Uterine fibroids are noncancerous growths that develop in or on the uterus, which affect many women at some point in their lives. These growths — also known as leiomyomas or myomas — are composed of muscle and fibrous tissue and can vary greatly in size. Some remain as small as a seed, while others can grow large enough to distort the shape of the uterus.
Although the vast majority of fibroids are benign, their impact ranges from unnoticed to significantly disruptive. Some women may have fibroids without experiencing symptoms, while others may struggle with severe menstrual bleeding, period cramps, or even fertility complications. Whether the fibroids result in significant symptoms depend on both their sizes and locations.
Types of Uterine Fibroids
Uterine fibroids are noncancerous, solid tumours made of muscle and fibrous tissue that develop within or on the uterus, which may cause symptoms such as heavy menstrual bleeding, period cramps, and pressure on surrounding organs.
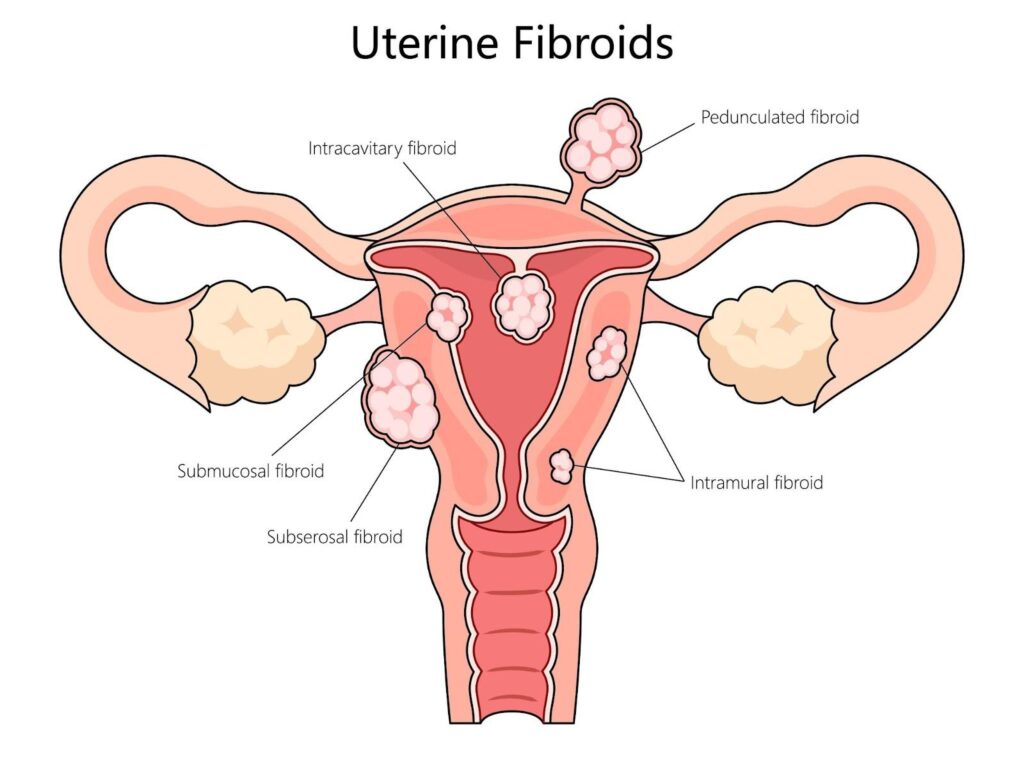
The location of fibroids within the uterus plays a key role in how they affect the body. The three primary types are:
Intramural Fibroids — the most common type, these grow within the muscular wall of the uterus. Small intramural fibroids can sometimes result in no symptoms; larger ones can cause heavy periods and/or pelvic discomfort as they expand [1].
Submucosal Fibroids — develop just beneath the lining of the uterus and extend into the uterine cavity [2]. Even small submucosal fibroids can lead to excessive menstrual bleeding and fertility issues.
Subserosal Fibroids — grow on the outer surface of the uterus. They typically can grow fairly large before they start resulting in symptoms, whereby they can sometimes press against adjacent organs like the bladder or intestines, leading to frequent urination or constipation [3].
Common Symptoms of Uterine Fibroids
While some fibroids remain asymptomatic, others can cause a range of symptoms depending on their size and location. The most common signs include:
Heavy and prolonged menstrual bleeding — fibroids can cause periods that last longer than usual or are excessively heavy, sometimes leading to (iron-deficiency) anaemia.
Pelvic pain and pressure — larger fibroids can create a sensation of fullness or pressure in the lower abdomen, leading to chronic discomfort.
Frequent urination — fibroids pressing against the bladder may cause an increased urge to urinate.
Constipation or bloating — subserosal fibroids that press against the intestines can disrupt digestion, causing bloating or difficulty passing stool or gas.
Difficulty in conceiving/ pregnancy complications — depending on their location/size, fibroids can cause difficulty in conceiving or pregnancy complications
(Rarely) Deep vein thrombosis (DVT) – should the uterus be grossly enlarged with multiple/sizable fibroid(s), vascular complications such as a DVT can result due to the fibroid uterus compressing on pelvic vessels
For many women, fibroids remain a silent condition, only discovered during routine gynaecological exams or health screening checks. However, if you experience symptoms that begin to interfere with daily life, it’s best to consult your gynaecologist for early diagnosis and management.
What Are Ovarian Cysts?
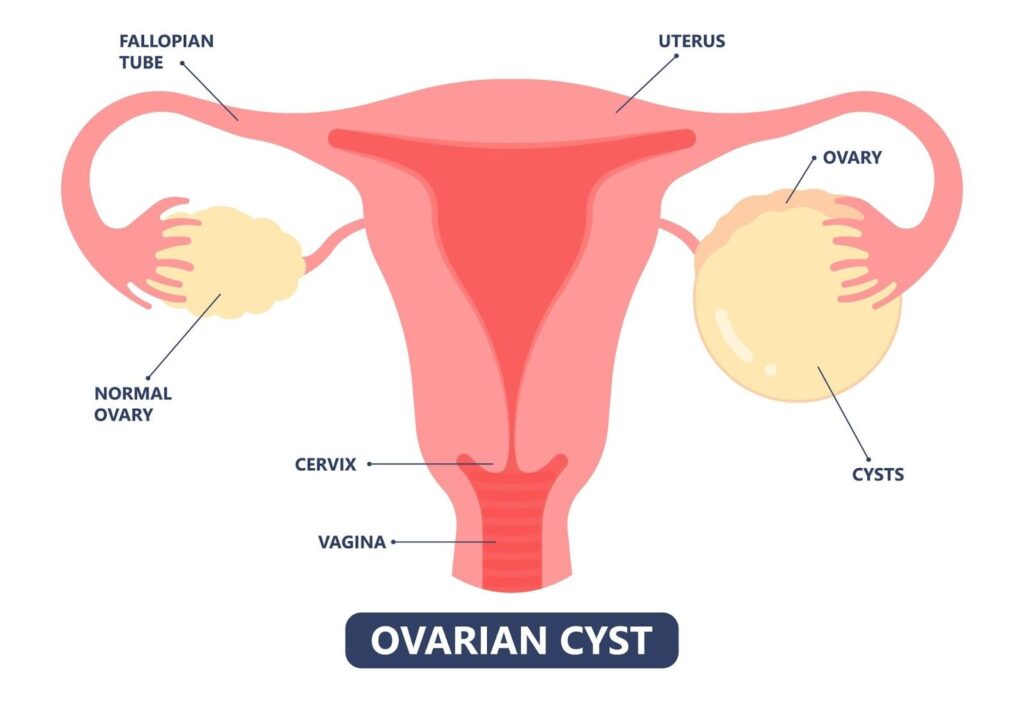
Ovarian cysts are fluid-filled sacs that develop in or on the ovaries. They are a common occurrence in women of reproductive age and, in many cases, remain harmless, causing no symptoms and disappearing on their own. However, some cysts grow larger, persist, or cause discomfort, leading to concerns about their impact on reproductive health and overall general health/ well-being.
Unlike uterine fibroids (which are solid growths of muscle and fibrous tissue), ovarian cysts are usually filled with fluid and can form due to various reasons. While most are benign, certain types may indicate underlying conditions that require medical intervention.
Types of Ovarian Cysts
Ovarian cysts are broadly classified into two main categories:
Functional Cysts — the most common type, these form as part of the normal menstrual cycle, are considered physiological and typically resolve on their own. All women in their reproductive lifespan will typically get these in their lifetimes. They include:
Follicular cysts — occur when a follicle fails to release an egg and continues to grow. These typically resolve after a few menstrual cycles and are harmless.
Corpus luteum cysts — this is a cyst that forms following ovulation (egg release), which produces progesterone in preparation for potential pregnancy. It can sometimes take a few menstrual cycles to fully resolve, and rarely may result in complications such as bleeding, causing transient pain.
Pathological Cysts — unrelated to the menstrual cycle, these cysts develop due to abnormal cell growth and may require medical attention. They include:
Dermoid cysts — formed from embryonic cells, containing tissue like hair, fat, or even teeth.
Endometriomas — caused by endometriosis, where uterine tissue grows outside the uterus and attaches to the ovaries, often leading to pain, distortion of pelvic anatomy, and fertility issues.
Cystadenomas — fluid-filled cysts that develop on the ovarian surface and can grow quite large.
Cancerous cysts – these are rare but are known to grow rapidly in size/ progress quickly with minimal symptoms. They commonly also have mixed solid-cystic areas within the cysts instead of being purely fluid-filled.
Ovarian cysts are fluid-filled sacs that develop in or on the ovaries, often resulting from hormonal changes or ovulation, sometimes causing pelvic pain, bloating, or menstrual irregularities.
Common Symptoms of Ovarian Cysts
Many ovarian cysts remain asymptomatic and are only discovered during routine pelvic examinations. However, when they become problematic, they can cause a variety of symptoms, including:
Pelvic pain — ranging from a dull ache to sharp, sudden pain, particularly if a large cyst ruptures, bleeds or twists, termed as an “ovarian cyst accident”.
Bloating or a feeling of fullness — larger cysts can cause abdominal discomfort or a sensation of heaviness/bloatedness.
Irregular menstrual cycles — some cysts interfere with normal ovulation, leading to unpredictable periods.
Pain during intercourse — cysts that exert pressure on surrounding tissues may cause discomfort or deep pain during sex.
Difficulty in conceiving — depending on their type, some ovarian cysts e.g. endometriomas can result in decreased ovarian reserve/function and therefore cause difficulty in conceiving.
Frequent urination or bowel issues — larger cysts can press against the bladder or intestines, leading to urinary urgency or constipation.
In rare cases, an ovarian cyst may rupture, bleed or become twisted (ovarian torsion). These situations require immediate medical attention. In cases of acute, severe pain, which can sometimes also be associated with nausea, fever etc, particularly if one has a known history of ovarian cyst, it is recommended to get evaluated at the nearest Accident and Emergency Department as urgent surgical intervention may sometimes be required before irreversible ovarian function loss occurs.
Cysts And Fibroids Are Vastly Different
Although both are common gynaecological conditions, they differ in structure, location, and how they affect the body. Fibroids are solid growths that develop in or on the uterus, while cysts are fluid-filled sacs that form in or on the ovaries. Their causes, symptoms, and treatment approaches also vary.
While some women may have both conditions at the same time, proper diagnosis through medical evaluation is essential to determine the most ideal course of action for managing symptoms and maintaining reproductive health.
The table below provides a clear comparison to help differentiate between the two:
Feature
Fibroids
Ovarian Cysts
Location
Develop in or on the uterus
Form in or on the ovaries
Composition
Solid, dense growths made of muscle and fibrous tissue
(Mostly) Fluid-filled sacs
Causes
Hormonal factors, genetics, and growth factors
Often linked to the menstrual cycle or hormonal imbalances
Common Symptoms
Heavy menstrual bleeding, pelvic pain, pressure symptoms such as frequent urination, constipation
Bloating, irregular periods, pelvic pain, pain during intercourse
Growth Pattern
Can grow gradually over time, sometimes reaching large sizes; does not resolve on their own. Typically stops growing when one reaches menopause and can start shrinking.
Can appear and disappear quickly, often resolving on their own
Impact on Menstruation
Causes prolonged or heavy periods
Can lead to irregular menstrual cycles
Potential Complications
May press on surrounding organs, leading to discomfort and fertility issues
May rupture or cause ovarian torsion, leading to sudden pain
While fibroids tend to develop slowly and may grow large before causing noticeable symptoms, ovarian cysts often come and go undetected. However, both conditions require medical evaluation if they cause persistent discomfort, affect menstrual cycles, or lead to fertility concerns.
Are Cysts or Fibroids Cancerous?
Most fibroids and cysts are benign, non-cancerous growths. In fact, many ovarian cysts resolve on their own, especially in premenopausal women.
However, in rare cases, certain forms of cysts, like complex ovarian cysts or rapidly growing fibroids, may raise some concern for malignancy. This is why it’s important to monitor these growths through regular check-ups with your doctor.
How Are Fibroids and Cysts Diagnosed?
The first step to treating your condition starts with an understanding of your condition. An accurate diagnosis is essential for distinguishing between fibroids and ovarian cysts, as their symptoms can sometimes overlap. While some women may not experience any noticeable signs, others may struggle with persistent pelvic pain, abnormal bleeding, or changes in their menstrual cycle.
Medical History and Physical Examination
Your gynaecologist may ask about:
The duration and severity of menstrual bleeding
The presence of pelvic pain, bloating, or pressure
Changes in urinary or bowel habits
Family history of fibroids or ovarian conditions
A physical examination, including a pelvic exam, helps detect any abnormalities in the uterus or ovaries. If a mass is present, further imaging tests are usually recommended to confirm the diagnosis and assess its characteristics.
Imaging Tests
To accurately identify whether a growth is a fibroid or a cyst, healthcare providers rely on imaging tests, including:
Ultrasound — the most commonly used diagnostic tool, ultrasound helps visualise both fibroids and cysts. A transabdominal ultrasound (performed over the abdomen) or a transvaginal ultrasound (inserted into the vagina for a closer view) can reveal the size, shape, and location of the growth. A transvaginal ultrasound is typically preferred over that of a transabdominal approach due to its proximity to the pelvic organs.
MRI (Magnetic Resonance Imaging) — provides more detailed images, particularly useful for fibroids. MRI scans help distinguish fibroids from other uterine conditions and determine the most suitable course of treatment.
Additional Tests — in some cases, further testing may be necessary to rule out complications or underlying conditions:
Blood Tests — women with heavy bleeding due to fibroids may be tested for anaemia and/or iron deficiency, which occurs when excessive blood loss reduces red blood cell levels.
Ovarian tumor marker blood tests e.g. CA-125 — used when a complex ovarian cyst is detected, blood tests such as tumor marker panels can measure CA-125 protein levels [4], which can be elevated in cases of ovarian cancer, endometriosis, or other conditions. However, an elevated CA-125 level does not necessarily indicate cancer (as it can also be raised in many benign or non-gynaecological conditions), and additional testing may be required for a definitive diagnosis.
Early detection helps prevent complications and allows for timely medical intervention for your symptoms.
How Do You Treat Fibroids and Cysts?
The management of fibroids and ovarian cysts depends on their size, symptoms, and potential complications. While many cases require only monitoring, others may need medical or surgical intervention. Below are the primary treatment approaches for both conditions.
Treatment for Fibroids
Not all fibroids require immediate treatment—many are small, asymptomatic, and discovered incidentally during routine gynaecological exams. For those that cause symptoms, the following options are available:
Observation — small, asymptomatic fibroids are often monitored through regular check-ups and imaging scans. If they do not grow or cause discomfort, no further treatment is necessary.
Medications — these range from non-hormonal medications (such as tranexamic acid/NSAIDs aka non-steroidal anti-inflammatory drugs, which can help alleviate heavy menstrual bleeding/menstrual cramps when taken on an as needed basis) to hormonal therapy, including birth control pills, progesterone-based treatments, or gonadotropin-releasing hormone (GnRH) agonists, can help reduce heavy bleeding, and alleviate symptoms [5]. However, these treatments do not eliminate nor shrink fibroids (other than GnRH injections, which can only be used for the short-term and hence does not serve to shrink fibroids effectively in the long-term).
Minimally Invasive Procedures — for women experiencing significant symptoms but wanting to avoid major surgery, procedures like uterine artery embolization (UAE) [6] or microwave ablation [7] can reduce fibroid size and symptoms by blocking their blood supply or using heat to destroy fibroid tissue. These, however, are usually temporalizing and typically do not have long-term efficacy and a proportion of women may ultimately require repeated procedures, hence precise case selection is required to determine suitability.
Surgical Options — for severe cases, surgery may be required:
Myomectomy — Myomectomyremoves fibroids while preserving the uterus, making it a preferred choice for women who wish to maintain fertility.
Hysterectomy — Hysterectomy involves removing the uterus entirely and is considered a definitive solution for recurrent or large fibroids in women who do not plan future pregnancies.
Treatment for Ovarian Cysts
Many ovarian cysts, particularly functional cysts, resolve on their own within a few menstrual cycles. However, when cysts persist, grow larger, or cause severe symptoms, treatment may be necessary.
Observation — functional cysts that are small and asymptomatic typically resolve naturally. Regular ultrasound monitoring ensures that they do not grow or develop complications.[8]
Medications — hormonal medications, such as birth control pills or progesterone-only medications, help prevent the formation of new functional cysts by regulating ovulation or suppressing ovarian activity. They can also sometimes shrink the size of existing ovarian cysts (depending on the nature).
Surgical Intervention — when a cyst becomes large, persistent, or causes significant symptoms, surgical removal may be required:
Cystectomy — Cystectomy removes only the cyst while preserving the ovary, which is ideal for benign cysts.
Oophorectomy — Oophorectomy removes the affected ovary if the cyst is large, complex, or suspected to be cancerous [9]. This option is considered when necessary to prevent complications.
Surgical intervention for an ovarian cyst has the potential to reduce one’s ovarian reserve and hence proper preoperative counseling is necessary for you to understand the implications of surgery and whether or not it is necessary for your case.
When to Visit a Gynaecologist
While many cases of fibroids and ovarian cysts do not cause serious issues, certain symptoms indicate the need for prompt medical evaluation. Seek immediate medical attention if you experience:
Severe or persistent pelvic pain — sudden, sharp pain may indicate a ruptured cyst or ovarian torsion, both of which require urgent care.
Heavy or prolonged menstrual bleeding — excessive blood loss from fibroids can lead to anaemia, causing fatigue, dizziness, and weakness.
Significant bloating or abdominal swelling — a rapidly growing fibroid or cyst may cause noticeable changes in the abdomen, warranting further investigation.
Pain during intercourse — persistent discomfort can be a sign of fibroids pressing on surrounding organs or cysts affecting the ovaries.
Changes in urination or bowel habits — frequent urination, constipation, or difficulty emptying the bladder may be due to large fibroids pressing against the bladder or intestines.
Unexplained weight changes or hormonal changes — symptoms like sudden weight changes, irregular periods, or excessive hair growth should not be overlooked.
Summary
Fibroids and ovarian cysts are two of the most common gynaecological conditions, yet they remain widely misunderstood. Many women only learn about them after experiencing symptoms like pelvic pain, heavy bleeding, or irregular periods. Others may have them without knowing, as these growths can sometimes develop silently. While fibroids and cysts share some similarities, they are fundamentally different in structure, causes, and the way they affect reproductive health.
Hopefully this quick guide helped shed some light on their differences, what to expect for each condition, and when to seek medical attention. If you’re experiencing unexplained pelvic pain, irregular periods, or other concerning symptoms, it is imperative to seek a gynaecologist’s opinion for a detailed diagnosis and personalised treatment plan.
Zhang, M., Cheng, S., Jin, Y., Zhao, Y., & Wang, Y. (2021). Roles of CA125 in diagnosis, prediction, and oncogenesis of ovarian cancer. Biochimica et Biophysica Acta (BBA) – Reviews on Cancer, 1875(2), 188503. https://doi.org/10.1016/j.bbcan.2021.188503
Uterine fibroids: Learn More – When is treatment with hormones considered? (2021). In InformedHealth.org [Internet]. Institute for Quality and Efficiency in Health Care (IQWiG). https://www.ncbi.nlm.nih.gov/books/NBK279532/
Lerardi AM, Savasi V, Angileri SA, Petrillo M, Sbaraini S, Pinto A, Hanozet F, Marconi AM, Carrafiello G. Percutaneous High Frequency Microwave Ablation of Uterine Fibroids: Systematic Review. Biomed Res Int. 2018 Jan 8;2018:2360107. doi: 10.1155/2018/2360107. PMID: 29511672; PMCID: PMC5817312.
Abdullah, B., Subramaniam, R., Omar, S., Wragg, P., Ramli, N., Wui, A., Lee, C., & Yusof, Y. (2010). Magnetic resonance-guided focused ultrasound surgery (Mrgfus) treatment for uterine fibroids. Biomedical Imaging and Intervention Journal, 6(2), e15. https://doi.org/10.2349/biij.6.2.e15
This article focuses on surgical treatment of endometriosis. Click here to find out about what endometriosis is, its symptoms and diagnosis.
How is endometriosis treated?
This depends on how severe your symptoms are, the stage of endometriosis, and your fertility plans. Endometriosis is a long-term condition. There is no cure and multiple surgeries are not recommended.. The aim of treatment is to achieve surgical clearance at the most appropriate time, with hormonal medicines before and after that to suppress endometriosis.
Surgery
Surgery is usually recommended for cases of advanced endometriosis with severe symptoms, or for women who wish to conceive soon but have difficulty getting pregnant. Depending on severity, a pre-operative MRI and a colorectal surgeon may need to be involved with your surgery.
Laparoscopy (keyhole) surgery under general anaesthesia allows for removal of endometriosis – this usually involves a 1cm cut in your umbilicus and three to four 0.5cm cuts in your abdomen. A laparoscope (camera) is inserted through your umbilicus and the extent of endometriosis determined. If there are endometriotic or “chocolate”/”blood” cysts in your ovaries, these will be removed (ovarian cystectomy). Endometriotic deposits in your pelvis will also be excised. Rarely, in severe cases where there is deep infiltrating endometriosis, the colorectal surgeon may need to perform shaving of endometriosis from the bowel or bowel resection (removing the section of bowel that has been affected by endometriosis).
If you are planning for pregnancy, additional procedures such as hysteroscopy to check your uterine cavity, hydrotubation (a dye test to check patency of your fallopian tubes) and ovariopexy (fixing your ovaries low down in the pelvis for better access during egg collection for in-vitro fertilisation) may be recommended.
Laparoscopic surgery for endometriosis is technically challenging due to long-term inflammation and scarring that the condition has caused – this usually results in adhesions between the intestines and pelvic organs. Anti-adhesion barriers (special bio-compatible materials) are typically placed at the end of the surgery to reduce the risk of adhesion reforming. In some cases, a laparoscopic procedure may need to be converted to a laparotomy (open) surgery. You will need to be hospitalised after the operation as it is a major surgery. Do discuss with your doctor who will be able to advise you on the risks of surgery in your specific case, and what to expect.
Hormonal medications to suppress endometriosis will need to be taken long-term, even if surgery has been done to clear endometriosis, unless you are trying to get pregnant, are pregnant or have reached menopause.
PMS refers to physical and emotional symptoms that affect your life 2 weeks before your period comes. These usually improve when your period starts and generally disappear by the time your period ends. PMS is usually linked to your body’s hormonal changes.
What are the symptoms of PMS?
Symptoms vary vastly depending on the woman. They include:
You should record your symptoms in a diary for at least 2-3 months to track their pattern, and see a gynaecologist if you find that your symptoms are worsening and/or interferes with your daily life.
What are the treatment for PMS?
There are many good ways to keep your symptoms under control so that your life does not revolve around your period. Some treatment options include:
Diet and vitamins Keeping a food diary is important to find out foods that trigger your symptoms. You may need to eliminate the foods that you suspect may be responsible from your diet and try them one at a time to see which one triggers your symptoms. Vitamin B6 has been shown to help with PMS.
Stress management Relaxation techniques, meditation, acupuncture, music, regular exercise can help relieve symptoms.
Psychological support These can be very useful for women suffering from chronic pelvic pain as this long-term condition can be debilitating and affect one’s relationships and quality of life. Cognitive behavioural therapy (CBT), where you discuss your symptoms with a therapist, can help PMS.
Non-hormonal medications These are anti-depressants (selective serotonin reuptake inhibitors (SSRIs) and serotonin–noradrenaline reuptake inhibitors (SNRIs). Your gynaecologist may prescribe these to be taken 2 weeks before your periods, or throughout your cycle.
Hormonal medications The first line is usually combined birth control pills (containing both estrogen and progesterone). The newer generation ones containing drospirenone (Yasmin, Yaz) has been shown to help PMS and should be taken continuously for better relief of symptoms. Other forms of hormonal medications include estrogen patches with oral progesterone/Mirena IUD. In severe cases, suppressive hormonal injections with add-back hormone replacement therapy can be considered.
Surgery This is reserved for the most severe cases of PMS which do not show improvement with all the above measures. Hormone replacement therapy will be needed after operation if surgery to remove the uterus and ovaries is done before 45 years old.
Why do I have bad menstrual cramps?
Menstrual cramps are lower abdominal aches and pains which many women may experience just before or during their periods. The pain can extend to your lower back, hips and inner thighs. Menstrual cramps occur because of uterine contractions during your period – strong contractions can cut off oxygen supply to your uterus and causes pain.
Bad or severe menstrual cramps may last throughout the period or linger on even when the period is over. Associated symptoms may include heavy periods, upset stomach, vomiting or loose stools.
If you have bad menstrual cramps that persist and is not relieved by normal painkillers, do see your gynaecologist as it may be a sign of something wrong.
What are some causes of bad menstrual cramps?
Endometriosis This is a condition where tissue from the womb lining is found outside the womb, most commonly in the pelvis, where it can affect the ovaries, fallopian tubes and intestines. These tissues respond to hormonal changes and bleed during periods, causing pain, inflammation, scarring.
Uterine fibroids These are non-cancerous growths that come from the muscle layer of the uterus (womb). They can result in the uterus to be larger than normal. Some fibroids can cause heavier periods than others depending on their location.
Adenomyosis This is a condition where the tissue from the womb lining grows into the muscle wall of the womb, causing the womb to be enlarged and resulting in heavy periods.
Pelvic inflammatory disease (PID) This is a condition where there is pain and inflammation of a woman’s uterus, fallopian tubes and ovaries, usually caused by sexually transmitted infections (STIs).
What tests do I need?
Your gynaecologist will take a detailed medical history and perform a pelvic examination to check your cervix and uterus. Depending on your symptoms, you may require an ultrasound scan, vaginal swabs or blood tests.
How to treat bad menstrual cramps?
This depends on what the cause of your cramps is. You should speak to your gynaecologist about the treatment options suitable for your condition. These may include:
Painkillers: Panadol, non-steroidal anti-inflammatory drugs (NSAIDs) to be taken as soon as the bleeding/pain starts
Heat pack: place this on your lower abdomen or back
Lifestyle changes: rest, avoid smoking and drinking, massage, regular exercise, stress management, traditional Chinese methods such as acupuncture
Hormonal medications: this can range from oral tablets (e.g. birth control pills, Visanne), implants (IUD, implanon) and injections
This article focuses on medical treatment of endometriosis. Click here to find out about what endometriosis is, its symptoms and diagnosis.
How is endometriosis treated?
This depends on how severe your symptoms are, the stage of endometriosis, and your fertility plans. Endometriosis is a long-term condition. There is no cure and multiple surgeries are not recommended. The aim of treatment is to achieve surgical clearance at the most appropriate time, with hormonal medicines before and after that to suppress endometriosis.
Medical treatment
These suppress the symptoms of endometriosis and slow down its disease progression (i.e. slows down the deposit of endometriosis outside the uterus). They are hormones which need to be taken long-term, even if surgery has been done to clear endometriosis, unless you are trying to get pregnant, are pregnant or have reached menopause. This is because endometriosis is thought to be related to backflow of menstrual blood every month, leading to tissue from the womb lining being found outside the womb. This means that endometriosis has a high chance of recurring even after surgical clearance has been done if suppressive medications are not taken post-operatively.
Common options include:
Visanne is commonly prescribed, and is an oral progestogen (1 pill daily) which reduces the pain and inflammation of endometriotic tissue. Women on Visanne either do not have periods, or more commonly experience irregular/prolonged spotting or bleeding. Visanne does not have birth control effects and women taking it need to use alternative birth control if they are not intending to get pregnant.
Mirenaintrauterine device (IUD) is a hormone device that can be inserted in the clinic. It lasts for 5 years and has a local effect by releasing progestogen slowly from its location in the uterus. Women using Mirena may have very light periods or none at all. It also acts as a birth control method.
Birth control pills (OCPs): this is an oral combined estrogen/progesterone pill taken daily. It is best taken continuously until breakthrough bleeding occurs, following which a short 4-day pill-free break can be taken before resuming daily pill-taking. This also acts as a birth control method.
Other forms may include progestogens in the form of injections – your doctor will discuss with you if you are suitable for it.
If you have advanced endometriosis with severe symptoms, or wish to conceive soon but have difficulty getting pregnant, you may require surgery.
Is my period long?
A normal period has bleeding that generally lasts between 3 to 7 days. Anything that goes beyond that is considered a prolonged period.
What can cause long periods?
Puberty or perimenopause Being at the extreme ends of reproductive age can cause periods to be erratic due to transition.
Hormone medications Certain birth control methods can cause long periods e.g. intrauterine contraceptive devices (IUD), implanon, injections (depo provera). Hormone medications such as Visanne (used to treat endometriosis) can also result in long (but light) periods.
Pregnancy Miscarriage or ectopic pregnancy can result in prolonged bleeding that can be mistaken as a long period.
Uterine fibroids These are non-cancerous growths that come from the muscle layer of the uterus (womb). They can result in the uterus to be larger than normal. Some fibroids can cause heavy and long periods depending on their location.
Endometrial polyps These are growths are attached to the lining of the uterus (endometrial lining) and result in long periods due to the disturbance of the womb lining.
Adenomyosis This is a condition where the tissue from the womb lining grows into the muscle wall of the womb, causing the womb to be enlarged and resulting in heavy long periods.
Pelvic inflammatory disease (PID) This is a condition where there is inflammation of a woman’s uterus, fallopian tubes and ovaries, usually caused by sexually transmitted infections (STIs).
Endometrial hyperplasia/ cancer or cervical cancer These may also have other symptoms like heavy periods, bleeding in between periods, bleeding after sex, or bleeding after menopause.
Bleeding disorders Certain bleeding disorders with reduced ability to clot may result in long periods.
Thyroid problems
When should I be concerned?
See your gynaecologist if you experience more than a few months of long periods, or have associated symptoms like heavy periods, bleeding in between periods, bleeding after sex, or bleeding after menopause.
What tests do I need?
Your gynaecologist will take a detailed medical history and perform a pelvic examination to check your cervix and uterus. Depending on your symptoms, you may require an ultrasound scan, pregnancy test, Pap smear/HPV test, vaginal swabs, biopsy of the womb lining, or blood tests.
Is there treatment for long periods?
Treatment depends on the cause for your long periods. If the cause is due to certain hormonal medications you are on and your tests return negative, you may not need to do anything if the flow is light. Discuss with your gynaecologist about the appropriate options for you.
What is chronic pelvic pain?
This refers to pain in the pelvis that lasts for 6 months or longer. In many cases there is no single cause for chronic pelvic pain, and the goal is pain management and improving one’s quality of life.
What are the symptoms of chronic pelvic pain?
Symptoms vary vastly depending on the woman. They include:
Pain that is present all the time
Pain that comes and goes
Dull achy feeling
Sharp pains
Pelvic heaviness
Painful sex
Bladder pain, or pain on urinating
Pain on sitting or standing for long periods of time
You should see a gynaecologist if you find that your pain is worsening and/or interferes with your daily life.
What are the causes of chronic pelvic pain?
This is usually a complex entity – sometimes pain can be from several conditions at once. Some causes include:
Endometriosis Tissue from the womb lining is found outside the womb, most commonly in the pelvis, where it can affect the ovaries, fallopian tubes and intestines. These tissues respond to hormonal changes and bleed during periods, causing pain, inflammation, scarring.
Bladder pain syndrome This is a condition of bladder discomfort or pain associated with urinary symptoms which can manifest in chronic pelvic pain.
Pelvic inflammatory disease (PID) This is a condition where there is inflammation of a woman’s uterus, fallopian tubes and ovaries, usually caused by an infection that spreads upwards from the vagina and cervix. Partially treated or chronic/recurrent PID can result in chronic pelvic pain due to scarring.
Musculoskeletal Conditions affecting the bones, joints, ligaments and muscles that make up the pelvis e.g. degeneration or inflammation may lead to chronic pelvic pain. Vulvodynia, which refers to chronic pain in the vulva, can also be a cause.
Ovarian remnant This occurs in women with history of surgery to remove their uterus and ovaries, whereby a small piece of ovary may be inadvertently left inside and cause painful symptoms.
Uterine fibroids These are non-cancerous growths that come from the muscle layer of the uterus (womb), and can cause painful periods which occasionally stretch into chronic pelvic pain. They frequently co-exist with endometriosis and adenomyosis.
Adenomyosis This is a condition where the tissue from the womb lining grows into the muscle wall of the uterus. This tissue respond to hormonal changes and continue to bleed (inside the uterine wall) during periods, causing painful periods which occasionally stretch into chronic pelvic pain. They frequently co-exist with endometriosis and uterine fibroids.
Irritable bowel syndrome Symptoms like chronic constipation, diarrhea and abdominal bloating can cause chronic pelvic pain.
Pelvic congestion syndrome This is where there are enlarged, dilated pelvic vessels around your uterus and ovaries. This is a common finding on scans and although most women with this do not experience any pain, in some women this may be attributed as the cause of their chronic pelvic pain.
Psychological Sometimes, depression, stress, being affected by other medical conditions or a history of physical or sexual abuse can result in chronic pelvic pain.
What tests do I need?
Your gynaecologist will take a detailed medical history and perform a pelvic examination to check for a possible cause for your pain.
Depending on your symptoms, you may require an ultrasound to check your uterus and ovaries, vaginal swabs to rule out sexually transmitted infections (STIs), urine tests to look for urinary tract infections, and/or bladder scan (to check the amount of urine remaining in your bladder after you have passed urine).
What is the treatment for chronic pelvic pain?
This depends on the cause. Finding a cause can be a long process and in some cases, a clear cause may not be found. Although there may not be a single cure available, communicating openly with your gynaecologist, pain specialist, family members and friends will enable you to find many good ways to keep your symptoms under control so that your life does not revolve around your pelvic pain.
Some treatment options include:
Diet Keeping a food diary is important to find out foods that trigger your symptoms. You may need to eliminate the foods that you suspect may be worsening your pain from your diet and try them one at a time to see which one triggers your symptoms. Smoking may worsen symptoms so try to quit smoking.
Stress management Relaxation techniques, meditation, acupuncture, music, regular exercise can help relieve symptoms.
Painkillers Simple painkillers like panadol and non-steroidal anti-inflammatory drugs (ponstan, synflex, ibuprofen) can help manage pain as needed. Long-term chronic pain may need referral to a pain specialist.
Physical therapy Stretching, massage and working with a specialised physiotherapist can help you identify specific points that trigger pain and develop coping strategies. One option for vulvodynia is trigger point therapy, where pressure is applied on trigger points for release. Another option is biofeedback or transcutaneous electrical nerve stimulation (TENS). In severe cases, numbing injections can be given by a pain specialist/anaesthetist.
Hormone medications This can be useful if the symptoms of chronic pelvic pain are related to the menstrual cycle as it can help to suppress ovulation and periods to get relief from pain symptoms.
Anti-depressants, psychological counselling These can be very useful for women suffering from chronic pelvic pain as this long-term condition can be debilitating and affect one’s self-esteem and quality of life.
Read more on the treatment for endometriosis, bladder pain syndrome, pelvic inflammatory disease, uterine fibroids and adenomyosis.
Remember that chronic pelvic pain is a chronic, long-term condition. Although there is no single cure available, there are many good ways to keep your symptoms under control so that your life does not revolve around your pain.
What is intermenstrual bleeding (IMB)?
This is bleeding or spotting that occurs in between your periods. Most women may experience this at some point.
Why am I experiencing bleeding in between my periods?
Pregnancy Miscarriage, ectopic pregnancy and implantation bleeding can be some of the pregnancy-related causes.
Ovulation This happens mid-cycle around ovulation, where women may have spotting for a few days. This is usually harmless, but if it persists, do see your gynaecologist.
Hormonal Pubertal or perimenopausal women may experience IMB due to hormonal changes.
Infections Sexually transmitted infections (STIs) like chlamydia and gonorrhea can cause IMB. Associated symptoms may include bleeding after sex, painful sex, abnormal vaginal discharge and fever.
Medications Hormone medications or implants may cause IMB especially in the starting phase. This includes birth control pills (especially if you miss pills), implants (IUD, implanon), hormone replacement therapy (HRT) or injections.
Uterine (endometrial) polyps These are growths are attached to the lining of the uterus (endometrial lining).
Uterine fibroids These are non-cancerous growths that come from the muscle layer of the uterus (womb). Fibroids that cause IMB are located near or at the lining of the uterus.
Abnormal uterine lining These include pre-cancer (endometrial hyperplasia) and endometrial cancer.
Endometriosis This is a condition where tissue from the womb lining is found outside the womb, most commonly in the pelvis, where it can affect the ovaries, fallopian tubes and intestines.
Cervical cancer This is usually associated with a lack of cervical screening and bleeding after sex.
When should I see my gynaecologist?
If the IMB occurs more than a few times within a month, or happens for a few months
Your gynaecologist will take a detailed medical history and perform a pelvic examination to check your cervix and uterus. Depending on your symptoms, you may require an ultrasound scan, vaginal swabs, Pap smear/ HPV test, biopsy of the womb lining or blood tests.
How to treat IMB?
This depends on what the cause of your IMB is. You should speak to your gynaecologist about the treatment options suitable for your condition. These may include:
Birth control pills: these eliminate ovulation and helps rule out mid-cycle ovulatory bleeding as a cause
Changing hormonal medications (if you are already on)
Antibiotics: for infection
Surgery: for structural causes like fibroids or uterine polyps
Why do I have bleeding after sex?
Bleeding after sex, or post-coital bleeding (PCB) can be fairly common, but should be checked out by a gynaecologist as it may be a sign of something wrong. Some causes include:
Cervical polyps or ectropion Cervical polyps are small growths that can occur on the cervix. Majority are non-cancerous and can be removed in the clinic. Ectropion is where cells that line the inside of the cervix grow on the outside – these are more sensitive and can bleed on contact.
Infections These can range from vaginal infections to sexually transmitted infections (STIs) causing pelvic inflammatory disease (PID) to genital warts.
Pelvic organ prolapse This refers to a drooping of the uterus, bladder or rectum beyond the vagina, and is more common in older women with previous childbirth.
Friction during sex Lack of foreplay, rough sex or sex toys can result in insufficient vaginal lubrication.
Pregnancy changes During pregnancy, there is increased blood supply to the cervix and bleeding can occur more easily after sex.
Vaginal atrophy Women who have menopaused have low estrogen which causes thin and dry vaginal skin that cracks easily.
Cervical cancer This is rare, but is usually associated with a lack of cervical screening.
What tests do I need?
Your gynaecologist will take a detailed medical history and perform a pelvic examination to check your cervix and uterus. Depending on your symptoms, you may require an ultrasound scan, vaginal swabs, Pap smear/HPV test, biopsy of the womb lining or blood tests.
How to treat bleeding after sex?
This depends on what the cause is. You should speak to your gynaecologist about the treatment options suitable for your condition. These may include:
Hormonal vaginal creams or tablets: topical vaginal estrogens for vaginal atrophy
What is postmenopausal bleeding (PMB)?
This is bleeding or spotting that occurs after menopause. Menopause means that you have not had a period in a year or more. You should see your gynaecologist promptly if you experience this.
Why am I experiencing bleeding after menopause?
Cervical polyps Cervical polyps are small growths that can occur on the cervix. Majority are non-cancerous and can be removed in the clinic.
Vaginal atrophy Women who have menopaused have low estrogen which causes thin and dry vaginal skin that cracks easily.
Pelvic organ prolapse This refers to a drooping of the uterus, bladder or rectum beyond the vagina, and is more common in older women with previous childbirth.
Uterine (endometrial) polyps These are growths are attached to the lining of the uterus (endometrial lining).
Abnormal uterine lining These include pre-cancer (endometrial hyperplasia) and endometrial cancer.
Cervical cancer This is rare, but is usually associated with a lack of cervical screening.
Medications Blood thinning medications e.g. warfarin, aspirin can cause you to be at increased risk of bleeding after menopause.
What tests do I need?
Your gynaecologist will take a detailed medical history and perform a pelvic examination to check your cervix and uterus. Depending on your symptoms, you may require an ultrasound scan, Pap smear/ HPV test, biopsy of the womb lining or blood tests.
How to treat PMB?
This depends on what the cause of your PMB is. You should speak to your gynaecologist about the treatment options suitable for your condition. These may include:
Hormonal vaginal creams or tablets: topical vaginal estrogensfor vaginal atrophy
Pelvic floor exercises, vaginal ring pessaries, surgery: for pelvic organ prolapse
Surgery: for polyps
Dr. Ng Kai Lyn
MBBS (SG) | MMed (SG) | MRCOG (UK) | FAMS (SG)
Empowering Women's Health
This article has been medically reviewed by Dr Ng Kai Lyn
Dr Ng Kai Lyn 黄楷伶 is a Consultant Obstetrician and Gynaecologist with sub-specialty expertise in urogynaecology and minimally invasive surgery, as well as a clinical interest in fertility.
The contents on this website provides general information only and does not replace professional or specialist advice. If you think you may have any medical condition, always seek prompt medical attention from a professional healthcare provider. It is not advisable to delay consulting professional advice by relying on the information provided here. Although reasonable efforts have been made to ensure that the information is relevant and comprehensive, we make no guarantees or representation that the contents on this website are complete, up-to-date or accurate. drngkailyn.com is independently owned and is not affiliated or endorsed by any organisation.








{kind=link}